Heliobas Disciple
TB Fanatic
Despite awareness of COVID-19 risks, many Americans say they're back to 'normal'
Many Americans know of the potential risks to themselves and their families from infection with COVID-19, but growing numbers say they have returned to living their "normal" pre-pandemic lives, according to July 2022 national survey data from the Annenberg Public Policy Center (APPC).
Despite awareness of COVID-19 risks, many Americans say they're back to 'normal'
by University of Pennsylvania
August 15, 2022

Credit: University of Pennsylvania
Many Americans know of the potential risks to themselves and their families from infection with COVID-19, but growing numbers say they have returned to living their "normal" pre-pandemic lives, according to July 2022 national survey data from the Annenberg Public Policy Center (APPC).
Increasing numbers say they personally know someone who has died from COVID-19 and personally know someone who has suffered the lingering effects such as neurological problems and fatigue that are commonly known as "long COVID," according to the APPC survey, which was conducted July 12–18, 2022.
Despite awareness of the continuing risks of COVID-19, worries about its health effects have declined, the percentage of Americans who often or always wear masks indoors with people from outside their household has plummeted, and the number saying they have returned to living their "normal, pre-COVID-19 life" has more than doubled over the past six months.
The nationally representative panel of 1,580 U.S. adults, surveyed by SSRS for the Annenberg Public Policy Center of the University of Pennsylvania, was the seventh wave of the Annenberg Science Knowledge (ASK) survey whose respondents were first empaneled in April 2021. The margin of sampling error (MOE) is ± 3.3 percentage points at the 95% confidence level. All changes noted in this release from previous surveys are statistically significant. See the appendix and methodology for additional information, including the survey questions.
Highlights
The survey, conducted amid a surge in cases of the coronavirus BA.5 omicron subvariant and spreading cases of monkeypox, found that:
- Over half of Americans (54%) personally know at least one person who has died of COVID-19.
- Nearly 1 in 3 (31%) know someone who has experienced long COVID.
- Most of the public knows someone who has tested positive for COVID-19 despite being fully vaccinated—or being fully vaccinated and boosted.
- A majority of Americans (54%) say they rarely or never wear a mask indoors when with people from outside their household—more than double the proportion in January.
- 4 in 10 (41%) say they have already returned to their "normal, pre-COVID-19 life"—up from 16% in January.
COVID-19 and vaccinations
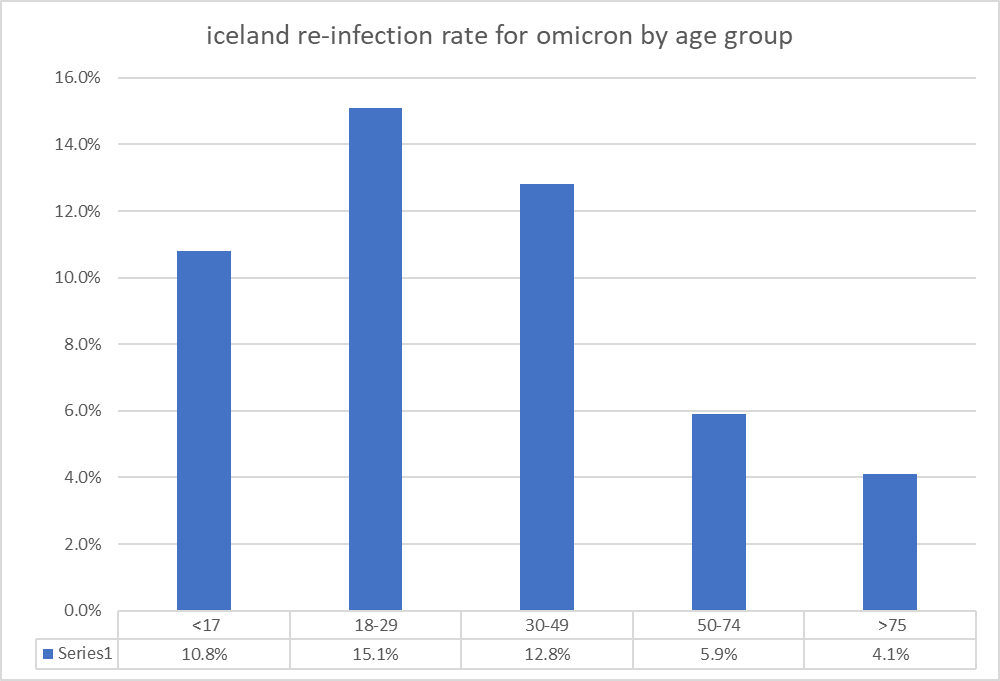
How many have had COVID: Over half of those surveyed (54%) say they tested positive for COVID-19 or were "pretty sure they had it" at some point since the first April 2021 wave of the survey, and 17% of those individuals, about 9% of the overall adult population, report having had it more than once.
Vaxxed and boosted: Nearly 4 in 5 (78%) Americans report being fully vaccinated against COVID-19, an increase from November 2021 (74%). Fully vaccinated means having had at least two doses of the Pfizer-BioNTech or Moderna vaccines or one dose of the Johnson & Johnson vaccine.
- Among the vaccinated, 77% have received a booster shot. In other words, 59% of U.S. adults overall say they're fully vaccinated against COVID-19 and have received a booster.
- Most of those (65%) who report being boosted have received one booster shot, while 35% have received two boosters.
Over half of those surveyed (53%) think it is likely that an individual who is vaccinated but not boosted will contract COVID-19 in the next three months.
A decline in health worries over COVID-19
As we noted in a July 29 news release, nearly 1 in 3 Americans (30%) are worried about getting COVID in the next three months, compared with nearly 1 in 5 (19%) who are worried about contracting monkeypox.
In July, fewer people worried that the health of family members will be seriously affected by having COVID-19 than in January 2022, though the public remains evenly divided between those who are and are not worried:
- About half of those surveyed (49%) are not worried that the health of someone in their family will be seriously affected from getting the coronavirus (up from 38% in January).
- And about half (48%) are worried that the health of family members will be seriously affected by contracting the coronavirus (down from 58% in January.)
59% are not worried that their own health will be seriously affected from getting the novel coronavirus, while 39% are worried.
And fewer people think hospitalization will be needed for unvaccinated individuals who contract COVID than previously:
Just over a third of those surveyed (36%) think that a sizable number of the unvaccinated ("21 percent or more") will require hospitalization if they get COVID, down from 45% in January and 51% in November 2021. A growing number (63%) think just a small portion of the unvaccinated ("20 percent or less") will need hospitalization if they get COVID-19.
A growing portion of the public (71%, up from 64% in April 2022) knows that long COVID—the long-term harmful effects such as neurological problems and fatigue that may ensue after having COVID-19—is caused by having COVID-19, though some people are still unsure. One in 5 people (22%, down from 29% in April) aren't sure that COVID-19 is the cause.

Credit: University of Pennsylvania
- Nearly a third of those surveyed (31%) say they know someone who has experienced long COVID, up from 24% in January.
- But fewer worry about actually getting long COVID—40% worry they will get long COVID if they are infected with COVID-19, down from 47% in January.
Treating COVID-19 with Paxlovid
Although the Food and Drug Administration (FDA) has authorized the use of an oral antiviral medication called Paxlovid to treat COVID-19, a substantial majority of those we surveyed had little or no familiarity with it. The survey finds that 4 out of 5 people (79%) are not at all or not too familiar with Paxlovid, including over half (54%) who say they are not at all familiar with it.
Among those who have some familiarity with Paxlovid (including individuals who say they are very, somewhat, and not too familiar), 61% regard it as a "safe and effective treatment" for COVID-19, while 11% considered it "safe but ineffective." Paxlovid is authorized for treatment of "mild to moderate cases" of COVID-19 in patients who are at "high risk for progression" to severe COVID-19, including hospitalization or death, according to the FDA.
Breakthrough infections among the vaccinated
The CDC says that COVID-19 vaccines "help prevent against severe illness, hospitalization, and death" but people "who are vaccinated may still get COVID-19." Most of the public knows about the occurrence of these so-called breakthrough infections, according to the Annenberg survey.
- Nearly two-thirds of those surveyed (64%) say someone who is fully vaccinated against COVID is still somewhat or very likely to contract the disease, up from 55% in April.
- Over half of those surveyed (56%) know someone who tested positive for COVID-19 even though that person was fully vaccinated against COVID but had not received a booster shot—up from 49% in April.
- Over two-thirds of those surveyed (68%) know someone who tested positive for COVID-19 even though that person was fully vaccinated and had received a booster shot—up from 49% in April.
- A majority of those surveyed (57%) disagree with the idea that breakthrough infections are evidence that COVID-19 vaccines don't work. Under a quarter (23%) of survey respondents see breakthrough infections as evidence COVID-19 vaccines don't work.
A decline in masking
Despite the risks from COVID-19, the Annenberg survey shows a sharp decline in the number of individuals who regularly wear masks to help protect themselves from getting COVID when they are in contact indoors with people who are not from their household.
"The wiliness of the newer subvariants and the realities that vaccinated immunity wanes and breakthrough infections can occur, among even those who are vaccinated and boosted, have increased the importance of other modes of protection," Jamieson noted. "These forms of protection include the use of high-quality, well-fitted masks when indoors with others who are not part of our households. Sadly, we are seeing a dramatic drop in this simple form of protection."
Asked if they wear a mask indoors when with other people who are not from their household:
- 54% say they never or rarely wear a mask, up from 46% in April and 25% in January. This is the first time a majority has said they never or rarely wear a mask since the question was first asked in September 2021.
- 43% sometimes, often, or always wear a mask, down from 51% in April and 72% in January.
- 43% agreed that everyone should be masked indoors (down from 60% in January) under those conditions.
- Over 1 in 3 people (36%) disagreed (up from 24% in January), meaning that they did not think everyone should be masked in such circumstances.
- And 21% neither agreed nor disagreed (up from 16% in January).
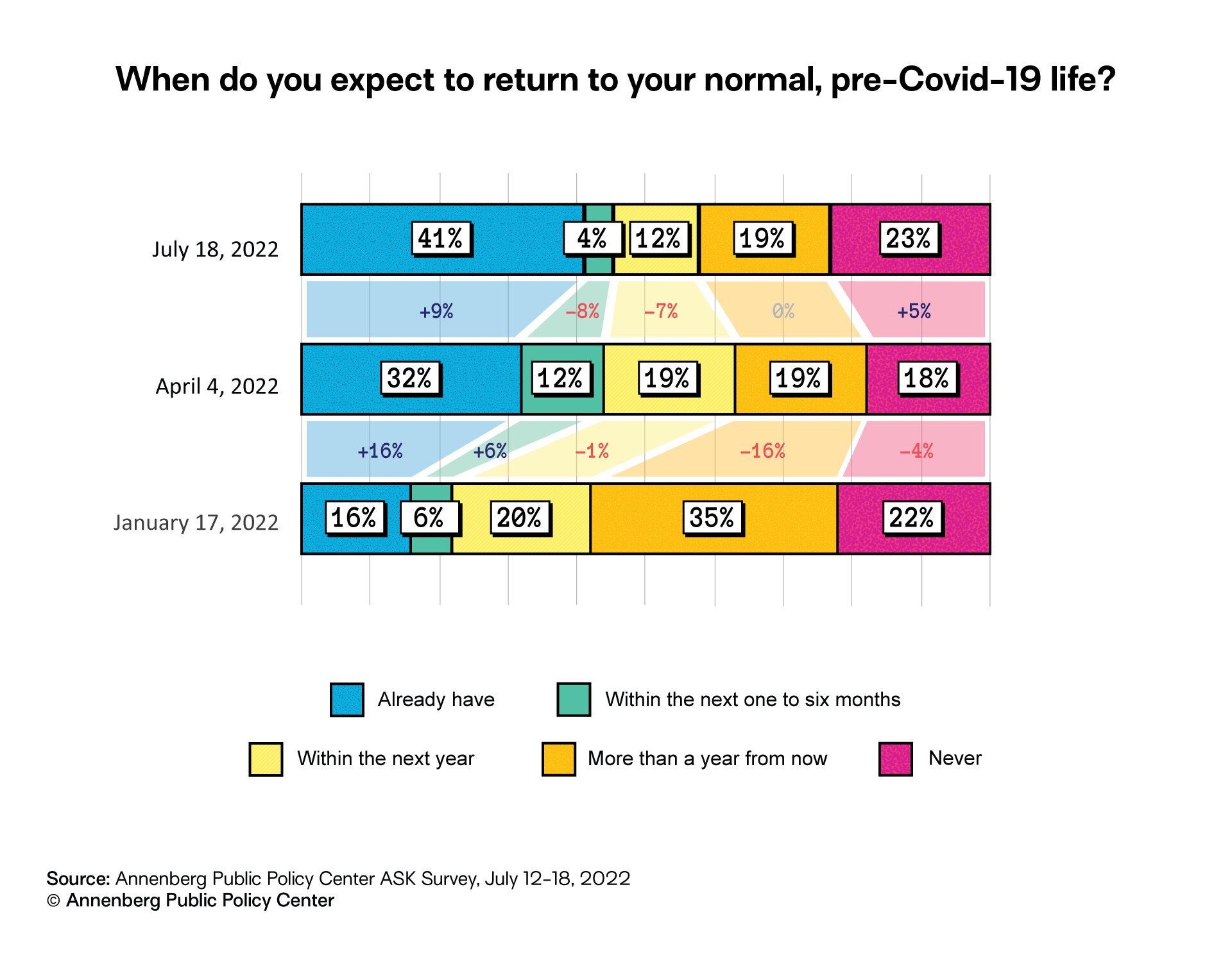
Asked when they expected to return to normal, 4 in 10 of the respondents said they already had. But sizable numbers think the return to normal remains a year away, or will never occur:
- 41% say they already have returned to normal, up from 32% in April and 16% in January.
- But 42% think the return to normal is still more than a year away (19%) or never (23%)—less than the 57% who were in those two groups in January.
A regression analysis conducted by APPC researchers finds that:
- Survey respondents who are men, who report being or leaning Republican, who say they aren't regularly wearing masks, or who indicate they are less worried about getting COVID in the next few months are more likely to say that they have already returned to normal.
- Respondents who are women, who say they are Democrats or lean Democratic, who are 65 and older, who regularly wear masks indoors around non-household members, or who are more worried about getting COVID in the next few months are less likely to report that they have already returned to normal.