Experts share their advice about isolation, masking and more if you're still testing positive late into a COVID-19 infection.

www.yahoo.com
(fair use applies)
Still Testing Positive for COVID-19 After 10 Days? What to Know
Sarah Jacoby - TODAY
Fri, July 29, 2022, 3:13 PM
We're in the midst of yet another wave of COVID-19 cases in the U.S., this one fueled by a subvariant of omicron
called BA.5. As COVID-19 continues to spread and new variants pop up, we'll need to keep relying on our go-to public health tools, including
at-home rapid antigen tests.
But the results from rapid tests — and how to act on them — can also be confusing, especially if you're still testing positive late in your infection.
Research from the Centers for Disease Control and Prevention indicates most people who have COVID-19 can expect to see
a positive result for five to nine days. But some people continue to get positive test results for even longer than that, and it's especially hard to know what to do in those circumstances.
Learn when to take a COVID-19 rapid test, how to interpret results and what to know about masking and isolating if you’re still testing positive at 10 days and beyond.
When should you take an at-home COVID-19 test?
In the event that you develop any symptoms that might signal COVID-19, you should take a home test immediately, the
CDC says.
Those symptoms — congestion, sore throat, cough, fever —
might be easily confused with other common illnesses, such as the flu, allergies or the common cold. But because we are still in the midst of a pandemic, it's a good idea to take a test to help rule out COVID-19 first, even if you may just be dealing with seasonal allergies.
If
you've been exposed to a close contact who has COVID-19, you should take a test at least five days after your last contact with that person. And if you test negative, consider taking another test one to two days later to help confirm your results, the CDC suggests.
As kids start to head back to school, rapid testing can be a particularly useful tool for keeping families and classmates safe experts
told TODAY. Isolating someone who tests positive is really the best way to halt a chain of transmission and keep the virus from spreading.
You can also take a test before attending an indoor gathering, especially if you know you won't be wearing a mask. Taking a rapid test can also help you determine whether to spend time with people who are particularly vulnerable to severe COVID-19 symptoms, like those with certain underlying health conditions.
The government is providing
at-home COVID-19 tests to Americans for free. Every household in the U.S. can now order up to
eight at-home rapid tests that get shipped directly to your address. The cost of other rapid tests should be
covered by health insurance, and tests may be available at community health centers for people who don’t have insurance.
And remember that even a
faint line on a home COVID-19 test should be considered positive. If you’re not sure whether or not your test is truly positive, you should check with your doctor, get a PCR test or
take a second rapid test the next day (and assume you really do have COVID-19 in the meantime).
What should you do if you test positive for COVID-19?
If you test positive for COVID-19, you should follow instructions from your doctor and the CDC about isolation. And you can end your isolation after just five days if you
never developed symptoms but should continue wearing a mask for a total of 10 days, according to the l
atest guidelines from the CDC.
Or, if you did develop symptoms, you can leave isolation after you've been without a fever for 24 hours (without using fever-reducing medication), provided your other symptoms are resolving as well. That can be as early as after five full days of isolation, the CDC says. Continue to mask around other people for another five days.
The CDC also amended its guidelines to add that, if you have access to a rapid antigen test, you can take the test at the end of day five of your isolation (as long as you've been fever-free for at least 24 hours without fever-reducing medication). If it's negative, you can use that result to feel more confident about leaving isolation at that time, but continue to mask. If it's positive, the CDC says you should continue isolating through day 10.
Regardless of when you end isolation, anyone who tests positive for COVID-19 should take precautions for 10 full days, the CDC says — including masking around others, avoiding travel and limiting contact with people who have a high risk for severe COVID-19.
If it's challenging to figure out what all those guidelines mean for your specific situation, take a look at the
CDC's new quarantine and isolation calculator tool.
How long do people normally test positive for COVID-19?
In the most general terms, people will likely test positive on an at-home rapid COVID-19 test for about six to 10 days, Dr. Stephen Kissler, a postdoctoral fellow at the Harvard T.H. Chan School of Public Health in the department of immunology and infectious diseases, told TODAY.
But with
PCR tests, which look for the virus's genetic material, people may test positive for even longer, Dr. Alberto Paniz-Mondolfi, associate professor at the Icahn School of Medicine at Mount Sinai, explained. "You can still have positivity that may persist for weeks and even months," he explained, noting that positive tests on PCR have been recorded for up to 60 days.
But there are a lot of factors that can affect how long someone may test positive.
Considering that different tests may perform differently “and then you have all these
variants, you’re changing the variables of the equation over and over again,” said Paniz-Mondolfi, who also leads the Saliva COVID Test Lab at Mount Sinai. That makes it difficult to predict exactly how many days someone will test positive.
Even with a rapid test, which detects molecules on the virus's surface as opposed to the virus's genetic material, it's not unheard of for people to test positive up to 14 days, especially for those who are unvaccinated, Kissler said. "We see a ton of variation between people in how long they test positive," he explained. "While that average is closer to six to 10 days, there are people who will hang on for longer than that."
Keep in mind that it's possible
to get COVID-19 more than once — even three or four times. So if there's a gap of weeks or months in between your positive tests, you might be dealing with a new infection.
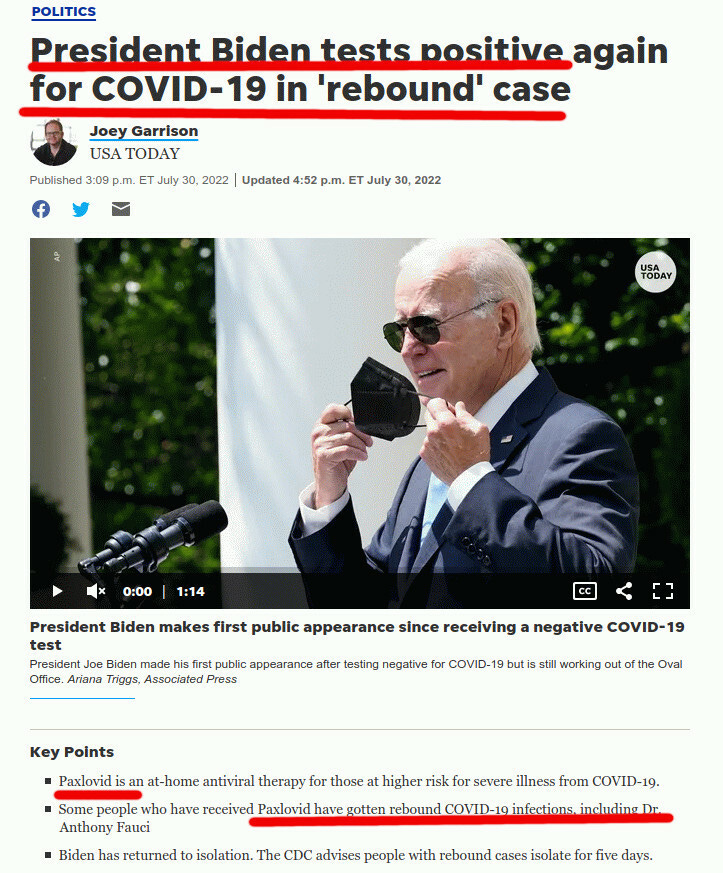
The use of at-home COVID-19 antiviral medications, like Paxlovid, may add another wrinkle: Some people are reporting that, after their symptoms resolve with treatment, the symptoms then return in a Paxlovid "rebound," Dr. Taison Bell, assistant professor of medicine at the University of Virginia, told
TODAY previously. Along with the return of COVID-19 symptoms, it's also possible to get another positive test — even if you tested negative just a few days earlier, the
CDC noted.
So, if you're trying to do your due diligence and testing at home frequently during your COVID-19 infection, know that it's possible for you to see positive results for a while.
Can you still be contagious after 10 days?
As long as you continue to test positive on a rapid at-home test, you should still consider yourself potentially contagious, Kissler said. But exactly how contagious you are “will change depending on where you are in the infection,” he explained.
In a
recent study published to a preprint server in April, researchers found that 17% of participants had active viral cultures beyond day five. Some had positive viral cultures for as long as 12 days after the onset of their symptoms, suggesting they could still be contagious.
But people tend to be most infectious right at the beginning of their COVID-19 infection. So by the time you reach day eight, nine or 10, “you still have the chance to spread to other people, but it’s probably not as much as you did early in the course of your infection,” Kissler said.
When you get to that point, you can start weighing your options. If it's essential that you start interacting with other people again (due to your job, for example), assess how you can do so as safely as possible.
If you're still testing positive late into your infection, what should you do?
The safest strategy is to continue to isolate until you're no longer testing positive, the experts stressed. But if you must interact with others before testing negative, make sure to wear a high-quality mask, maintain distance from other people when you can, and avoid spending time in enclosed spaces around other people.
But for people for whom that might not be feasible, it’s not unreasonable to gradually leave isolation — even if you’re still testing positive on a rapid test, Kissler said. That's especially true if you're fully vaccinated, any symptoms you developed have resolved, and you continue to take other precautions (especially masking) until you get a negative result.
“You might be able to begin slowly sort of reintegrating while still being mindful of your contact," Kissler said. If you're going to be around other people, he recommended avoiding enclosed spaces with others and wearing a mask (ideally an N95,
KN95 or KF94) when coming into contact with other people.
After 10 days, it's likely that "you're good to go, and you're even better to go if you keep practicing containment measures," Paniz-Mondolfi agreed. "Keep wearing your mask. Keep practicing social distancing."
And, of course, if you're concerned about how long you've been testing positive, check in with a health care provider for their guidance on your individual situation, Kissler said.







 Calling Geert and Dr. Alexander..
Calling Geert and Dr. Alexander..





























")