Double boosted Biden gets COVID, the latest and most public debunking of the narrative "the vaccinated won't get COVID." Vaccine-only prevention has failed, Paxlovid-only early Rx will too.

pierrekory.substack.com
(fair use applies)
My Fox News.Com Op-Ed On The President's Vaccine Failure
Double boosted Biden gets COVID, the latest and most public debunking of the narrative "the vaccinated won't get COVID." Vaccine-only prevention has failed, Paxlovid-only early Rx will too.
Pierre Kory, MD, MPA
17 hr ago
Big week of Op-Eds for me and the team! We got one
published in the Federalist last week, and we got
another one published on FoxNews.com two days ago (included below). I have been informed that foxnews.com is the 3rd most popular website on the internet. Whoa.
I used to be bothered by appearing on news sites with sometimes overt political affiliations. However, as a physician educator living during a historic period of unprecedented levels of scientific censorship, both me and the FLCCC long ago decided to publish and speak to any entity capable of widely disseminating the pragmatic, expert, and evidence-based guidance we have formulated for citizens. Whether you are blue, red, black, or brown etc, we want to help.
Now, Biden getting sick leaves the vaccinators clinging to the last remaining narrative used to combat their Public Enemy #1, that of “vaccine hesitancy” amongst the U.S. population. This last narrative is the famous “you won’t go to the hospital or die from COVID if you are vaccinated.” The original narrative that
vaccines protect against disease and spread was ultimately disproven (
section 2 in this prior post), but this one is a bit trickier. The only surprising fact about the first false narrative was how long they were able to cling to it using propaganda and absurd chicanery like when the CDC
recommended against testing the vaccinated (that one still shocks me in its brazenness). The even greater absurdity is that supposedly legal mandates persist for a vaccine that does not prevent transmission.
Yesterday Biden tested negative and unsurprisingly came out in a victory lap, extolling his administrations efforts against COVID, crediting boosters, at home tests, and the availability of “easy to use” effective treatments from our friends at Pfizer. Absurd misinformation from the nation’s top medical mis-informationist (takes one to know one apparently - wink, wink). He goes on to say, “you can take these pills at home and you can get them from tens of thousands of pharmacies.”
He then follows this with, “the PFDA (the P is not a typo) even put in a special rule so that pharmacists can
prescribe the drug!” Pharmacists don’t prescribe by the way (or at least never have in the past). He then exulted, “you don’t even have to go to the doctor!” Note he is referring to the distribution of Pfizer’s Paxlovid, a drug with
120 important drug interactions across 25 different classes of very commonly prescribed medications. It cannot be given concurrently with 75 of them and you have to adjust doses with an additional 29. Even Biden had to be taken off of two of his medications to be treated with it.
I have never in my career used a medication with this many complex drug interactions. Not even close. Yet, now in the U.S it will be “prescribed” by a pharmacist with no more than a superficial knowledge of the chronicity, severity, or treatment history of the patient’s other illnesses. The practice of medicine has been so stellar throughout COVID, this program will assuredly kick it up a notch via this novel direct delivery system of the Pfresident’s (the f is not a typo) pricey new pill. The United States of Pharma is alive and well.
View: https://www.youtube.com/watch?v=K8lkHREnWHw
23 min 50 sec
In the same little speech, he goes on to recommend that all kids over 5 should get vaccinated. Why not include the toddlers while you are at it Joe? I would have loved to be a fly on the wall during his team’s discussion of whether he should just “go for it all” and include the toddlers. I mean the PFDA and CDC unanimously authorized it’s EUA on what is essentially zero evidence to support one (if anything, the trials data, correctly interpreted, indicate negative benefits to toddlers). Yet two large committees, staffed with “Gods of Science and Knowledge” supported a recommendation for use in this age group. Unanimously.
I personally think he didn’t mention toddlers due to the fact that only 2-3% of American parents have brought them in for COVID vaccination. I trust that History will not be kind to this little press conference of misinformation.
So, the vaccinators are now down to their last narrative supporting the vaccines as below (not the one about the vaccinated going to heaven, the one above that).

The “vaccine knowledgeable” minority of the public is small, but the data contradicting this narrative is immense. The U.S is the only country with “official” data to support this assertion, however that data has been so covertly manipulated, almost none of the general public or health system providers are aware of the manipulation nor how it was accomplished.
In previous posts, (
here and
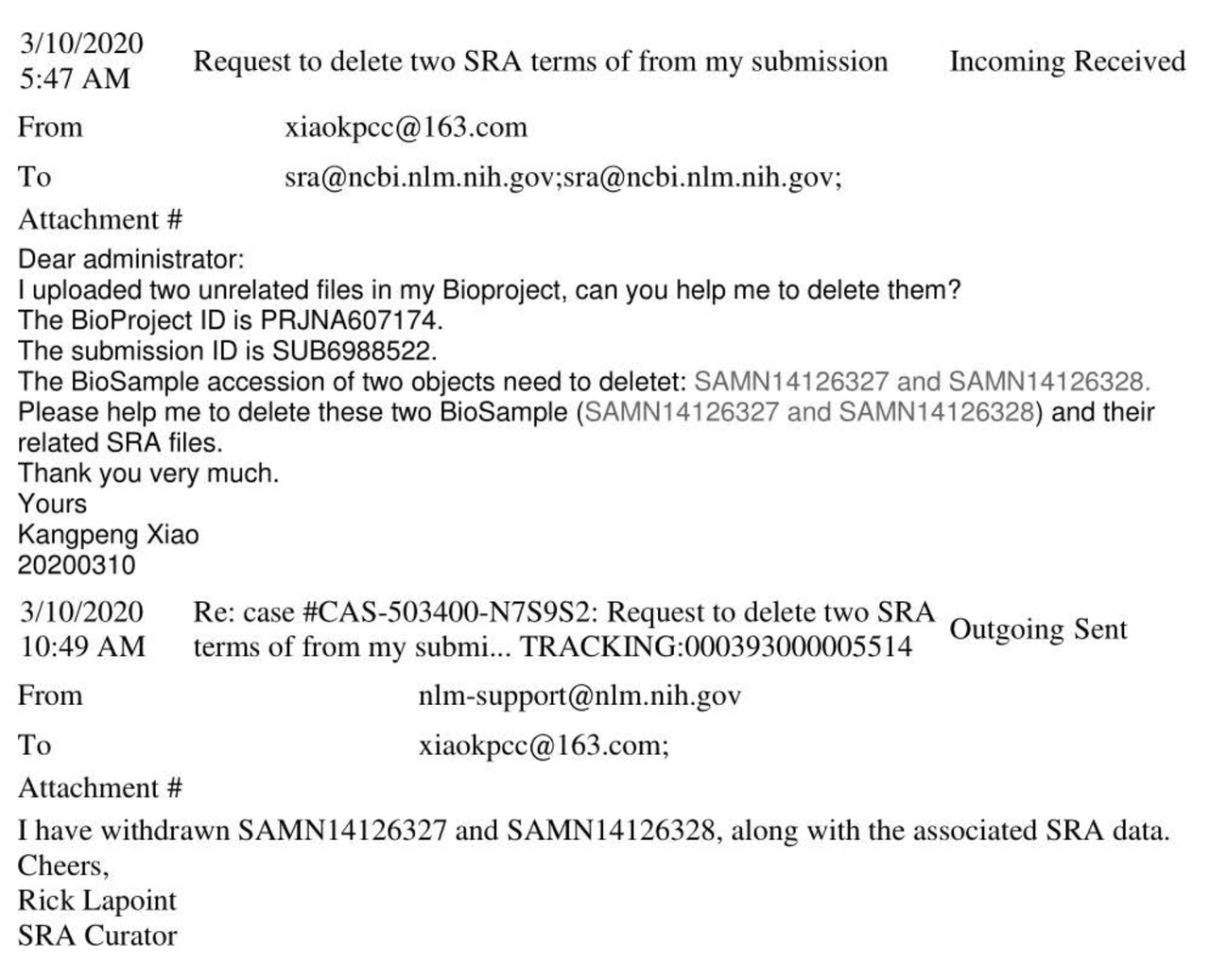
here), I explored my hypothesis of a systematic and faulty documentation of vaccination status in most U.S hospitals. I recently received further confirmation of its existence. My main front-line nurse source for those two prior posts informed me this weekend that at her academic medical center, she started pointing out to senior nursing colleagues that the majority of patients are listed in the medical record as “unvaccinated” or “unknown” despite the fact that proof of their COVID-19 vaccination is in the chart (albeit buried in a nursing admission note which does not electronically flag them as being vaccinated). It should be noted that no other vaccination was documented in this fashion prior to COVID.
As a result of her “educational” intervention, many senior nurses and nursing directors are now aware of this “glitch.” So much so that it is now openly talked about in staff meetings where nurses and physicians are now being instructed on how to find the actual COVID vaccination status of a hospitalized patient. The reason why staff are so interested in finding out the vaccination status is to better understand the possible causes of the the myriad complex illness presentations they are seeing as well as the increased rates of unprecedented and catastrophic medical emergencies being seen in young, healthy patients ( heart attacks, strokes, aggressive cancers etc). Previously many staff were under the impression that such presentations were due to “long covid”, whereas now they are seeing the truth - that these are the horrible sequelae of COVID mRNA vaccination with lipid nanoparticles.
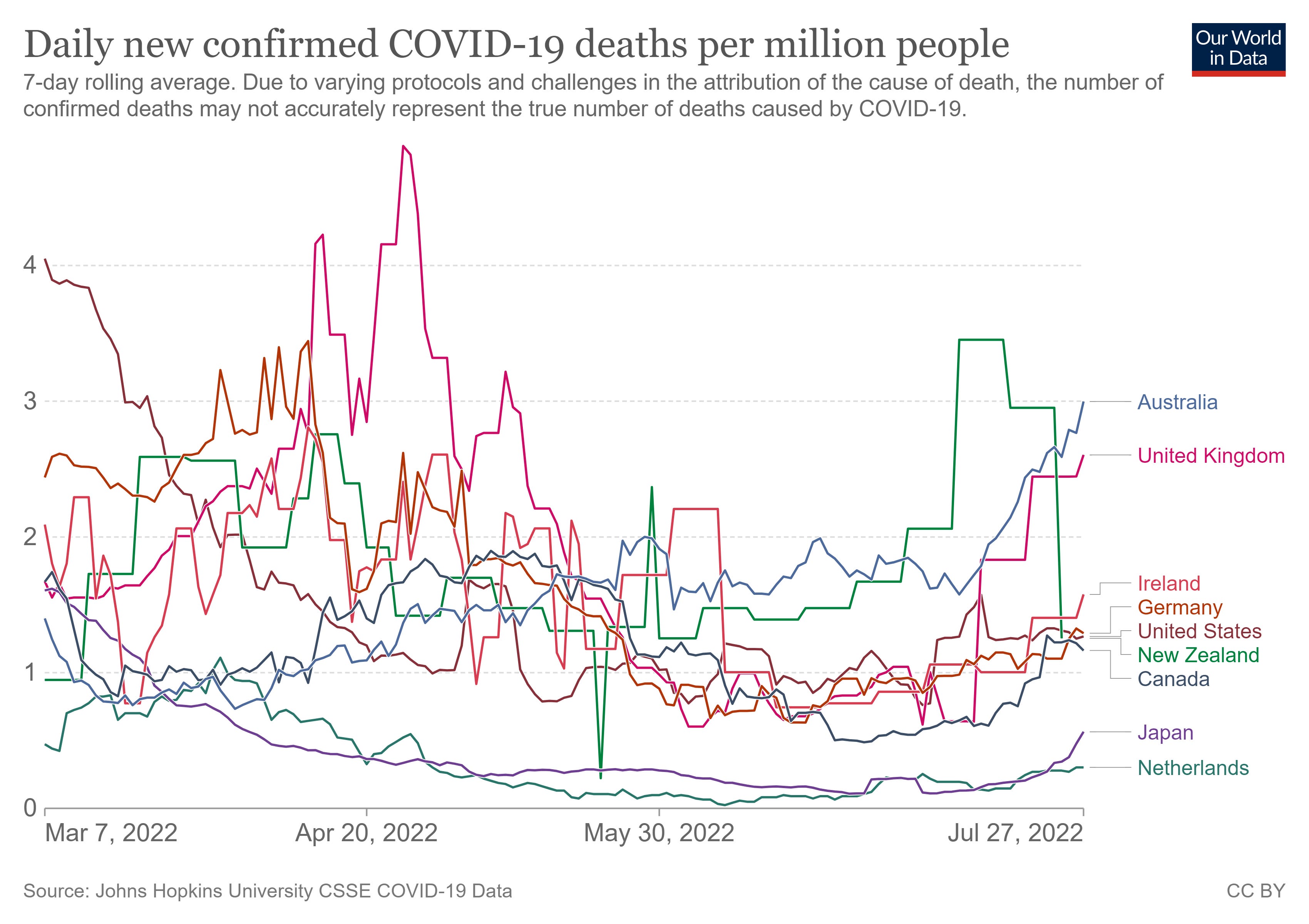
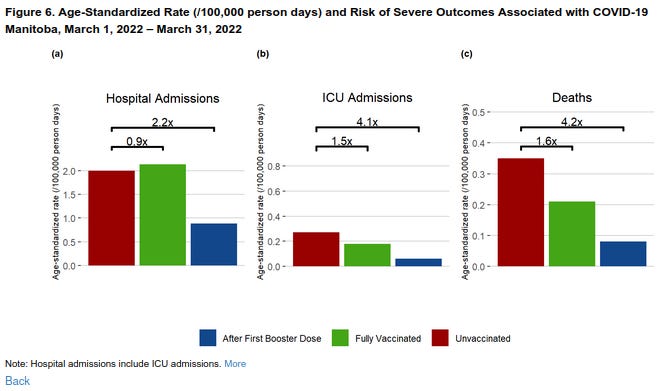
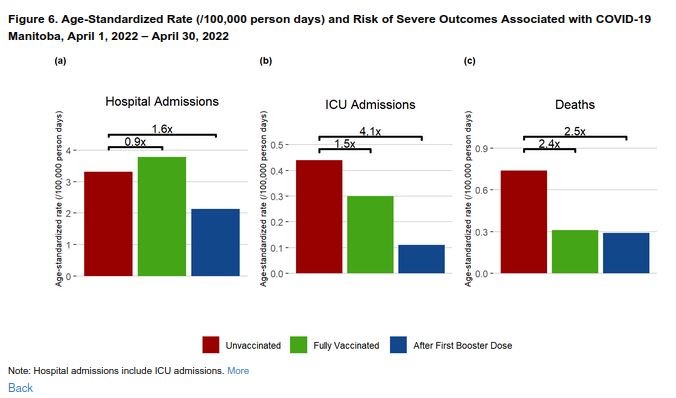
It is my impression that this systems “glitch” (an investigative journalist I know is trying to find the source of it) compromises the entirety of the U.S hospital data used by the CDC to support this last narrative. Looking at data from countries that did not have this process baked into their electronic medical record-keeping, you find the rates of vaccinated entering hospitals and dying have far
exceeded the rates of the unvaccinated for many months now (see Section 3 in
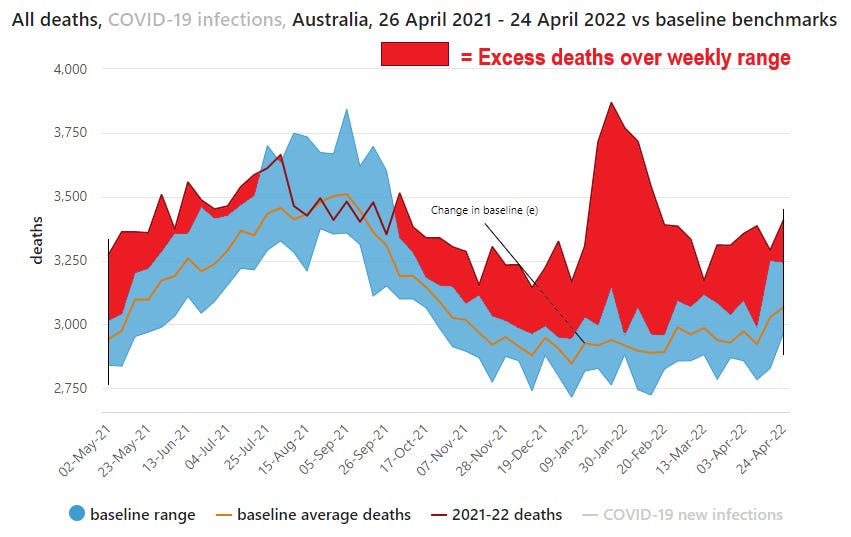
this prior post of mine for the data supporting this). The most recent and striking example
are the data coming out of New South Wales in Australia showing;
- Of the 798 COVID deaths in the last 8 weeks, all but 2 were vaccinated
- Of the 142 deaths in the last week, all were vaccinated, 68% were boosted.
Anyway, on to my Op-Ed where I again, for the millionth time, essentially plead for a more pragmatic and effective approach to the pandemic, one based on an early treatment initiative using safe, repurposed medications. This time I highlighted the evidence for fluvoxamine (had to get off the ivermectin and hydroxychloroquine beat).
Ideally, I think a national campaign of checking every American’s Vitamin D level followed by supplementation strategies to achieve a level above 50 ng/ml for all would have the greatest impact in mitigating the morbidity and mortality of COVID. Maybe I will save that for my next Op-Ed. Enjoy:
OPINION
Published July 26, 2022 7:00am EDT
Biden's COVID-19 diagnosis is proof vaccines aren't enough to fight virus
Fighting virus requires new tools because vaccines aren't enough and Biden diagnosis is proof
By
Pierre Kory
President Joe Biden’s COVID-19 diagnosis is the latest data point showing our government’s "vaccine only" approach needs an immediate course correction. If four doses of a vaccine cannot protect the leader of the free world from infection, it is time to consider other tactics.
These measures should include generic medicines that have been dismissed by the mainstream medical community and media.
While Americans across the ideological spectrum wish the president a speedy recovery, we must take this moment to acknowledge that a strategy blindly focused on vaccinations is not getting the job done.
Don’t take my word for it. Use Biden’s own standard for success. Exactly one year before testing positive, the President declared, "You're
not going to get COVID if you have these vaccinations." Back then, the seven-day average of new cases in the United States was around 50,000. Today, that number is estimated to be between 300,000-500,000 when considering ubiquitous and uncounted home testing, despite two-thirds of the population considered "fully vaccinated" by the CDC.
Yet the push for vaccines from the administration has continued unabated. Following Biden’s diagnosis, the White House tried to take a political victory lap. In their first press briefing following news of the diagnosis, White House press secretary Karine Jean-Pierre stressed the president’s vaccination status as, "what’s most important here."
As a lifelong Democrat and medical doctor who has helped more than 700 patients recover from COVID-19 and its complications, I have seen the effectiveness of other treatment options with my own eyes. Take for instance, fluvoxamine, an inexpensive generic medicine typically associated with depression treatment. It costs $4 per pill, is readily available at pharmacies, and has demonstrated an effectiveness combating COVID-19 in large, randomized, controlled trials published in the Journal of the American Medical Association and the Lancet.
Yet two years after this data appeared, fluvoxamine is still getting the cold shoulder from the medical gatekeepers. Both the World Health Organization (WHO) and National Institutes of Health do not recommend its use against COVID-19.
Furthermore,
medical professionals who deviate from the party line are callously dismissed by mainstream media outlets such as NPR, as "fringe medical doctors, natural healers and internet personalities ready to push unproven cures for COVID."
 Video
Video
Science and medicine are always changing for the better. Consider the incredible shifts in the landscape that occurred between the current president contracting the novel coronavirus and his predecessor. In October 2020, there were limited options available for President Donald Trump. Less than two years later, a nearly 80-year-old president was presumed to be on a path toward recovery on the day of his diagnosis.
Progress is a wonderful thing, but it’s only possible with an attitude of open-mindedness that challenges the status quo. Doctors and innovators should be incentivized to pursue and explore new and different approaches. Instead, we are being forced to adopt a group think or risk suffering the wrath of the establishment, or worse, loss of livelihood.
The powerful American Board of Internal Medicine, a sprawling organization with certification authority, has been issuing threatening letters to board-certified physicians with exemplary careers, accusing them of "misinformation" when their public assessments of the efficacy of generic, repurposed therapies contradict those of federal health agencies.
To be sure, demonstrably false "misinformation" can be dangerous, and a topic worthy of discussion. But with overwhelming evidence to support the statements in question, advocating different courses of action toward COVID-19 is far from misinformation. In fact, the
suggestion from the White House that the vaccine lessened Biden’s symptoms more closely meets the standard for misinformation since it is an impossible standard to prove.
Of all people, Biden should be open to new ideas. He was elected with a clear mandate to implement a fresh approach toward the pandemic. Two summers ago, he castigated his predecessor, saying, "the president still does not have a plan."
He went on to say, "More than 170,000 Americans have died — by far the worst performance of any nation on Earth."
Today, that number has — sadly — topped 1 million. Many more lives have been lost on this president’s watch than the last one. These are sobering statistics. Biden has fallen short of promise to "shut down" the virus.
It’s clear COVID-19 is going to be with us for the foreseeable future. How we address it is up to us. Now is the time for a change in approach. Let’s hope our elected leaders and medical professionals take heed.
Pierre Kory, M.D., is President and Chief medical officer of the Front Line COVID-19 Critical Care Alliance.

 www.voiceforscienceandsolidarity.org
www.voiceforscienceandsolidarity.org