Heliobas Disciple
TB Fanatic
(fair use applies)
A call for an independent inquiry into the origin of the SARS-CoV-2 virus
Neil L. Harrison nh2298@columbia.edu and Jeffrey D. Sachs
May 19, 2022
Since the identification of theSARS-CoV-2 in Wuhan, China, in January 2020 (1), the origin of the virus has been a topic of intense scientific debate and public speculation. The two main hypotheses are that the virus emerged from human exposure to an infected animal [“zoonosis” (2)] or that it emerged in a research-related incident (3). The investigation into the origin of the virus has been made difficult by the lack of key evidence from the earliest days of the outbreak—there’s no doubt that greater transparency on the part of Chinese authorities would be enormously helpful. Nevertheless, we argue here that there is much important information that can be gleaned from US-based research institutions, information not yet made available for independent, transparent, and scientific scrutiny.
When it comes to deciphering the origins of COVID-19, much important information can be gleaned from US-based research institutions—information that has yet to be made available for independent, transparent, and scientific scrutiny.
The data available within the United States would explicitly include, but are not limited to, viral sequences gathered and held as part of the PREDICT project and other funded programs, as well as sequencing data and laboratory notebooks from US laboratories. We call on US government scientific agencies, most notably the NIH, to support a full, independent, and transparent investigation of the origins of SARS-CoV-2. This should take place, for example, within a tightly focused science-based bipartisan Congressional inquiry with full investigative powers, which would be able to ask important questions—but avoid misguided witch-hunts governed more by politics than by science.
Essential US Investigations
The US intelligence community (IC) was tasked, in 2021 by President Joe Biden (4), with investigating the origin of the virus. In their summary public statement, the IC writes that “all agencies assess that two hypotheses are plausible: natural exposure to an infected animal and a laboratory-associated incident” (4). The IC further writes that “China’s cooperation most likely would be needed to reach a conclusive assessment of the origins of COVID-19 [coronavirus disease 2019].” Of course, such cooperation is highly warranted and should be pursued by the US Government and the US scientific community. Yet, as outlined below, much could be learned by investigating US-supported and US-based work that was underway in collaboration with Wuhan-based institutions, including the Wuhan Institute of Virology (WIV), China. It is still not clear whether the IC investigated these US-supported and US-based activities. If it did, it has yet to make any of its findings available to the US scientific community for independent and transparent analysis and assessment. If, on the other hand, the IC did not investigate these US-supported and US-based activities, then it has fallen far short of conducting a comprehensive investigation.
This lack of an independent and transparent US-based scientific investigation has had four highly adverse consequences. First, public trust in the ability of US scientific institutions to govern the activities of US science in a responsible manner has been shaken. Second, the investigation of the origin of SARS-CoV-2 has become politicized within the US Congress (5); as a result, the inception of an independent and transparent investigation has been obstructed and delayed. Third, US researchers with deep knowledge of the possibilities of a laboratory-associated incident have not been enabled to share their expertise effectively. Fourth, the failure of NIH, one of the main funders of the US–China collaborative work, to facilitate the investigation into the origins of SARS-CoV-2 (4) has fostered distrust regarding US biodefense research activities.
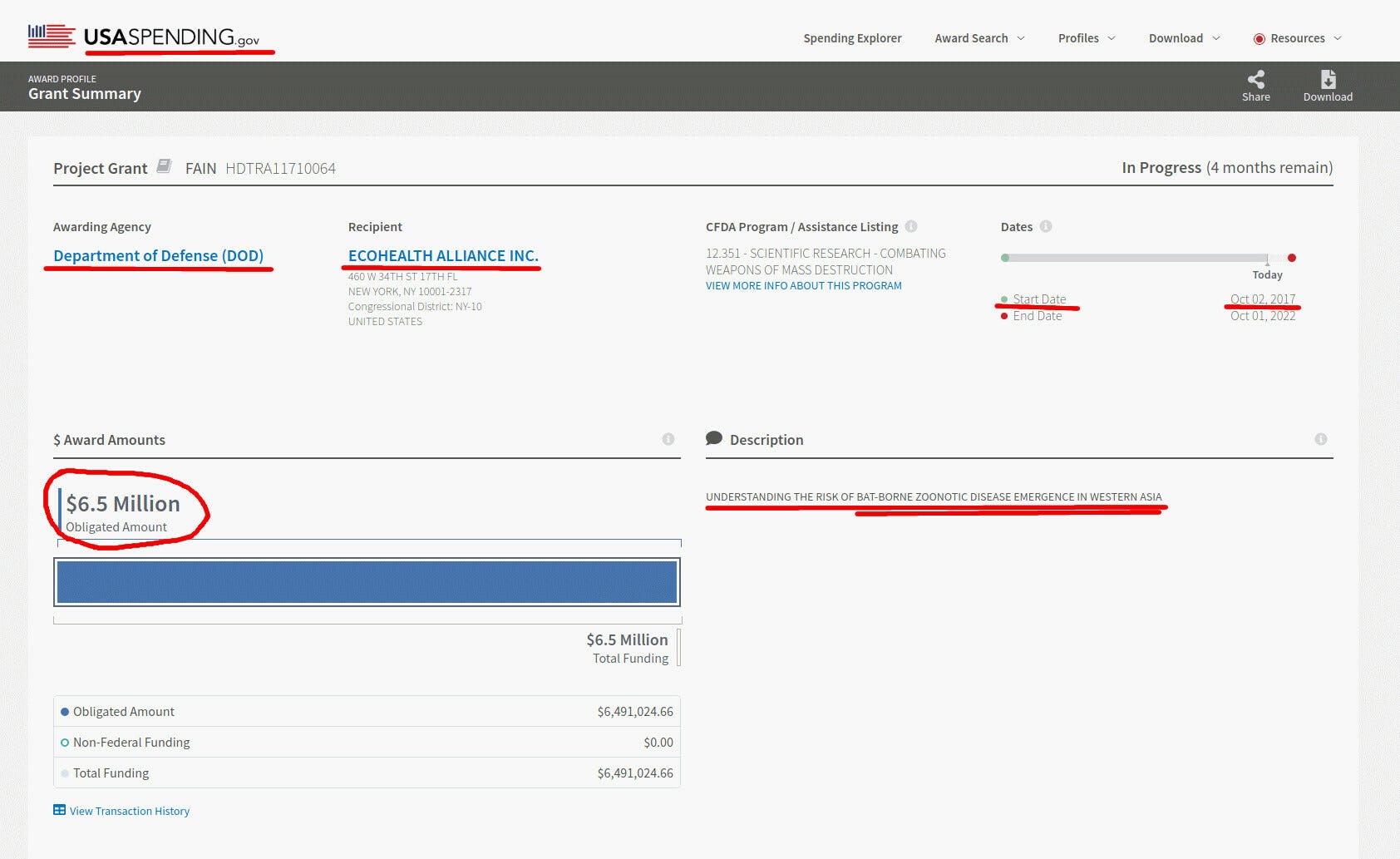
Much of the work on SARS-like CoVs performed in Wuhan was part of an active and highly collaborative US–China scientific research program funded by the US Government (NIH, Defense Threat Reduction Agency [DTRA], and US Agency for International Development [USAID]), coordinated by researchers at EcoHealth Alliance (EHA), but involving researchers at several other US institutions. For this reason, it is important that US institutions be transparent about any knowledge of the detailed activities that were underway in Wuhan and in the United States. The evidence may also suggest that research institutions in other countries were involved, and those too should be asked to submit relevant information (e.g., with respect to unpublished sequences).
Participating US institutions include the EHA, the University of North Carolina (UNC), the University of California at Davis (UCD), the NIH, and the USAID. Under a series of NIH grants and USAID contracts, EHA coordinated the collection of SARS-like bat CoVs from the field in southwest China and southeast Asia, the sequencing of these viruses, the archiving of these sequences (involving UCD), and the analysis and manipulation of these viruses (notably at UNC). A broad spectrum of coronavirus research work was done not only in Wuhan (including groups at Wuhan University and the Wuhan CDC, as well as WIV) but also in the United States. The exact details of the fieldwork and laboratory work of the EHA-WIV-UNC partnership, and the engagement of other institutions in the United States and China, has not been disclosed for independent analysis. The precise nature of the experiments that were conducted, including the full array of viruses collected from the field and the subsequent sequencing and manipulation of those viruses, remains unknown.
EHA, UNC, NIH, USAID, and other research partners have failed to disclose their activities to the US scientific community and the US public, instead declaring that they were not involved in any experiments that could have resulted in the emergence of SARS-CoV-2. The NIH has specifically stated (6) that there is a significant evolutionary distance between the published viral sequences and that of SARS-CoV-2 and that the pandemic virus could not have resulted from the work sponsored by NIH. Of course, this statement is only as good as the limited data on which it is based, and verification of this claim is dependent on gaining access to any other unpublished viral sequences that are deposited in relevant US and Chinese databases (7,8). On May 11, 2022, Acting NIH Director Lawrence Tabak testified before Congress that several such sequences in a US database were removed from public view, and that this was done at the request of both Chinese and US investigators.
Blanket denials from the NIH are no longer good enough. Although the NIH and USAID have strenuously resisted full disclosure of the details of the EHA-WIV-UNC work program, several documents leaked to the public or released through the Freedom of Information Act (FOIA) have raised concerns. These research proposals make clear that the EHA-WIV-UNC collaboration was involved in the collection of a large number of so-far undocumented SARS-like viruses and was engaged in their manipulation within biological safety level (BSL)-2 and BSL-3 laboratory facilities, raising concerns that an airborne virus might have infected a laboratory worker (9). A variety of scenarios have been discussed by others, including an infection that involved a natural virus collected from the field or perhaps an engineered virus manipulated in one of the laboratories (3).
Overlooked Details
Special concerns surround the presence of an unusual furin cleavage site (FCS) in SARS-CoV-2 (10) that augments the pathogenicity and transmissibility of the virus relative to related viruses like SARS-CoV-1 (11, 12). SARS-CoV-2 is, to date, the only identified member of the subgenus sarbecovirus that contains an FCS, although these are present in other coronaviruses (13, 14). A portion of the sequence of the spike protein of some of these viruses is illustrated in the alignment shown in Fig. 1, illustrating the unusual nature of the FCS and its apparent insertion in SARS-CoV-2 (15). From the first weeks after the genome sequence of SARS-CoV-2 became available, researchers have commented on the unexpected presence of the FCS within SARS-CoV-2—the implication being that SARS-CoV-2 might be a product of laboratory manipulation. In a review piece arguing against this possibility, it was asserted that the amino acid sequence of the FCS in SARS-CoV-2 is an unusual, nonstandard sequence for an FCS and that nobody in a laboratory would design such a novel FCS (13).
Fig. 1.

This alignment of the amino acid sequences of coronavirus spike proteins, in the region of the S1/S2 junction, illustrates the sequence of SARS-CoV-2 (Wuhan-Hu-1) and some of its closest relatives. The furin cleavage site (FCS) is indicated (PRRAR'SVAS), and furin cuts the spike protein between R and S, as indicated by the red arrowhead. Adapted from Chan & Zhan (15).
[CONTINUED NEXT POST]
A call for an independent inquiry into the origin of the SARS-CoV-2 virus
Neil L. Harrison nh2298@columbia.edu and Jeffrey D. Sachs
May 19, 2022
Since the identification of theSARS-CoV-2 in Wuhan, China, in January 2020 (1), the origin of the virus has been a topic of intense scientific debate and public speculation. The two main hypotheses are that the virus emerged from human exposure to an infected animal [“zoonosis” (2)] or that it emerged in a research-related incident (3). The investigation into the origin of the virus has been made difficult by the lack of key evidence from the earliest days of the outbreak—there’s no doubt that greater transparency on the part of Chinese authorities would be enormously helpful. Nevertheless, we argue here that there is much important information that can be gleaned from US-based research institutions, information not yet made available for independent, transparent, and scientific scrutiny.
When it comes to deciphering the origins of COVID-19, much important information can be gleaned from US-based research institutions—information that has yet to be made available for independent, transparent, and scientific scrutiny.
The data available within the United States would explicitly include, but are not limited to, viral sequences gathered and held as part of the PREDICT project and other funded programs, as well as sequencing data and laboratory notebooks from US laboratories. We call on US government scientific agencies, most notably the NIH, to support a full, independent, and transparent investigation of the origins of SARS-CoV-2. This should take place, for example, within a tightly focused science-based bipartisan Congressional inquiry with full investigative powers, which would be able to ask important questions—but avoid misguided witch-hunts governed more by politics than by science.
Essential US Investigations
The US intelligence community (IC) was tasked, in 2021 by President Joe Biden (4), with investigating the origin of the virus. In their summary public statement, the IC writes that “all agencies assess that two hypotheses are plausible: natural exposure to an infected animal and a laboratory-associated incident” (4). The IC further writes that “China’s cooperation most likely would be needed to reach a conclusive assessment of the origins of COVID-19 [coronavirus disease 2019].” Of course, such cooperation is highly warranted and should be pursued by the US Government and the US scientific community. Yet, as outlined below, much could be learned by investigating US-supported and US-based work that was underway in collaboration with Wuhan-based institutions, including the Wuhan Institute of Virology (WIV), China. It is still not clear whether the IC investigated these US-supported and US-based activities. If it did, it has yet to make any of its findings available to the US scientific community for independent and transparent analysis and assessment. If, on the other hand, the IC did not investigate these US-supported and US-based activities, then it has fallen far short of conducting a comprehensive investigation.
This lack of an independent and transparent US-based scientific investigation has had four highly adverse consequences. First, public trust in the ability of US scientific institutions to govern the activities of US science in a responsible manner has been shaken. Second, the investigation of the origin of SARS-CoV-2 has become politicized within the US Congress (5); as a result, the inception of an independent and transparent investigation has been obstructed and delayed. Third, US researchers with deep knowledge of the possibilities of a laboratory-associated incident have not been enabled to share their expertise effectively. Fourth, the failure of NIH, one of the main funders of the US–China collaborative work, to facilitate the investigation into the origins of SARS-CoV-2 (4) has fostered distrust regarding US biodefense research activities.
Much of the work on SARS-like CoVs performed in Wuhan was part of an active and highly collaborative US–China scientific research program funded by the US Government (NIH, Defense Threat Reduction Agency [DTRA], and US Agency for International Development [USAID]), coordinated by researchers at EcoHealth Alliance (EHA), but involving researchers at several other US institutions. For this reason, it is important that US institutions be transparent about any knowledge of the detailed activities that were underway in Wuhan and in the United States. The evidence may also suggest that research institutions in other countries were involved, and those too should be asked to submit relevant information (e.g., with respect to unpublished sequences).
Participating US institutions include the EHA, the University of North Carolina (UNC), the University of California at Davis (UCD), the NIH, and the USAID. Under a series of NIH grants and USAID contracts, EHA coordinated the collection of SARS-like bat CoVs from the field in southwest China and southeast Asia, the sequencing of these viruses, the archiving of these sequences (involving UCD), and the analysis and manipulation of these viruses (notably at UNC). A broad spectrum of coronavirus research work was done not only in Wuhan (including groups at Wuhan University and the Wuhan CDC, as well as WIV) but also in the United States. The exact details of the fieldwork and laboratory work of the EHA-WIV-UNC partnership, and the engagement of other institutions in the United States and China, has not been disclosed for independent analysis. The precise nature of the experiments that were conducted, including the full array of viruses collected from the field and the subsequent sequencing and manipulation of those viruses, remains unknown.
EHA, UNC, NIH, USAID, and other research partners have failed to disclose their activities to the US scientific community and the US public, instead declaring that they were not involved in any experiments that could have resulted in the emergence of SARS-CoV-2. The NIH has specifically stated (6) that there is a significant evolutionary distance between the published viral sequences and that of SARS-CoV-2 and that the pandemic virus could not have resulted from the work sponsored by NIH. Of course, this statement is only as good as the limited data on which it is based, and verification of this claim is dependent on gaining access to any other unpublished viral sequences that are deposited in relevant US and Chinese databases (7,8). On May 11, 2022, Acting NIH Director Lawrence Tabak testified before Congress that several such sequences in a US database were removed from public view, and that this was done at the request of both Chinese and US investigators.
Blanket denials from the NIH are no longer good enough. Although the NIH and USAID have strenuously resisted full disclosure of the details of the EHA-WIV-UNC work program, several documents leaked to the public or released through the Freedom of Information Act (FOIA) have raised concerns. These research proposals make clear that the EHA-WIV-UNC collaboration was involved in the collection of a large number of so-far undocumented SARS-like viruses and was engaged in their manipulation within biological safety level (BSL)-2 and BSL-3 laboratory facilities, raising concerns that an airborne virus might have infected a laboratory worker (9). A variety of scenarios have been discussed by others, including an infection that involved a natural virus collected from the field or perhaps an engineered virus manipulated in one of the laboratories (3).
Overlooked Details
Special concerns surround the presence of an unusual furin cleavage site (FCS) in SARS-CoV-2 (10) that augments the pathogenicity and transmissibility of the virus relative to related viruses like SARS-CoV-1 (11, 12). SARS-CoV-2 is, to date, the only identified member of the subgenus sarbecovirus that contains an FCS, although these are present in other coronaviruses (13, 14). A portion of the sequence of the spike protein of some of these viruses is illustrated in the alignment shown in Fig. 1, illustrating the unusual nature of the FCS and its apparent insertion in SARS-CoV-2 (15). From the first weeks after the genome sequence of SARS-CoV-2 became available, researchers have commented on the unexpected presence of the FCS within SARS-CoV-2—the implication being that SARS-CoV-2 might be a product of laboratory manipulation. In a review piece arguing against this possibility, it was asserted that the amino acid sequence of the FCS in SARS-CoV-2 is an unusual, nonstandard sequence for an FCS and that nobody in a laboratory would design such a novel FCS (13).
Fig. 1.
This alignment of the amino acid sequences of coronavirus spike proteins, in the region of the S1/S2 junction, illustrates the sequence of SARS-CoV-2 (Wuhan-Hu-1) and some of its closest relatives. The furin cleavage site (FCS) is indicated (PRRAR'SVAS), and furin cuts the spike protein between R and S, as indicated by the red arrowhead. Adapted from Chan & Zhan (15).
[CONTINUED NEXT POST]