Heliobas Disciple
TB Fanatic
Immune sensor ZBP1 links interferon treatment and dangerous inflammatory cell death during COVID-19
Scientists from St. Jude Children's Research Hospital have shown that the innate immune sensor, ZBP1, and its associated inflammatory cell death pathway, PANoptosis, are major contributors to the negative effects of interferon treatment and high interferon levels in some COVID-19 patients. The...
Immune sensor ZBP1 links interferon treatment and dangerous inflammatory cell death during COVID-19
by St. Jude Children's Research Hospital
May 19, 2022
Scientists from St. Jude Children's Research Hospital have shown that the innate immune sensor, ZBP1, and its associated inflammatory cell death pathway, PANoptosis, are major contributors to the negative effects of interferon treatment and high interferon levels in some COVID-19 patients. The work was published today in Science Immunology.
For viral infections, interferon therapy is a proposed treatment that should help the immune system efficiently clear viruses. But in patients with established SARS-CoV-2 infections, interferon therapy has produced mixed results, in some cases even increasing mortality, which appears to be mediated by ZBP1.
"Our study improves our fundamental understanding of innate immunity and inflammatory cell death pathways and shows how modulating these processes during coronavirus infection could be used to improve patient outcomes," said corresponding author Thirumala-Devi Kanneganti, Ph.D., St. Jude Department of Immunology vice-chair.
"Interferons induce the expression of interferon-stimulated genes. Some of these genes show antiviral function while some drive cell death," she said. "One such interferon-stimulated gene is ZBP1. Interferon induces robust expression of ZBP1, which can then sense SARS-CoV-2 and drive inflammatory cell death. This cell death is detrimental for patient outcomes."
Screening for a gene
The scientists wanted to find out which genes sensed SARS-CoV-2 and contributed the most to poor outcomes in COVID-19 patients treated with interferon. To find these genes, they used a CRISPR-Cas9 screen that knocked out genes in macrophages infected with coronavirus. Researchers then observed which genes were missing in the surviving cells. These genes were likely critical for sensing the virus and driving cell death, since their deletion resulted in the cells surviving the infection. This unbiased screening method identified ZBP1 as one such gene. ZBP1 was also expressed at higher levels in the immune cells of patients with worse outcomes during COVID-19 than those who fully recovered.
Kanneganti's group has been studying ZBP1 and its role in cell death for many years. The group initially identified ZBP1 as an innate immune sensor of influenza virus that activates PANoptosis. PANoptosis is an inflammatory cell death pathway discovered by Kanneganti's lab. It integrates components from—but is also distinct from—other cell death pathways such as pyroptosis, apoptosis and necroptosis.
ZBP1 is upregulated by interferon to sense and respond to viral infections. The researchers showed that deleting the gene ZBP1 in mice infected with coronavirus prevented cell death and mortality during interferon therapy. Additionally, cell death was prevented in human cells in response to SARS-CoV-2 infection by knocking down the expression of ZBP1.
Preventing inflammatory cytokine storms
The scientists showed that the body's antiviral inflammatory response was the cause of poor outcomes during coronavirus infection. The interferon response is a natural mechanism the immune system uses to combat infections. This response starts local inflammation at the site of viral infection to draw immune cells to the area and prevent viral spread.
Interferon also activates interferon-stimulated genes such as ZBP1 that cause cell death to prevent viral spread. In patients with poor outcomes, this response becomes uncontrolled. Cell death causes the production of cytokines, powerful immune signaling molecules. Cytokine production causes more cell death, which causes more cytokine production. This cycle creates a positive feedback loop that ultimately leads to a dangerous immune event known as a cytokine storm.
Cytokines are produced in large quantities during a cytokine storm, causing an overreaction throughout the body. This overreaction activates signaling cascades that cause serious issues, including multi-organ failure. Cytokine storms are connected to COVID-19 severity and mortality.
An overstimulated cell death pathway
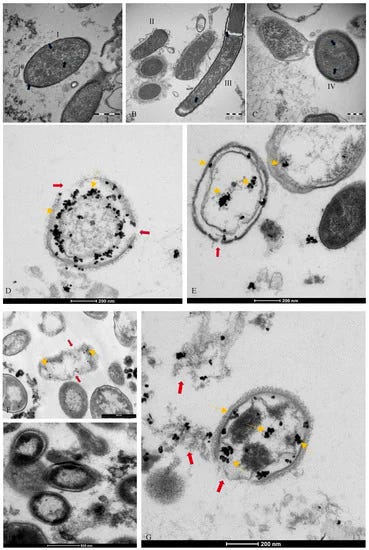
The group documented that the proteins associated with inflammatory cell death, PANoptosis, were activated in SARS-CoV-2-infected macrophages treated with interferon, compared to untreated macrophages. The researchers found similar results when coronavirus-infected mice were treated with interferon. The cell death was accompanied by the release of proinflammatory cytokines. This provided the researchers with a mechanistic understanding of how ZBP1 could lead to a cytokine storm during a coronavirus infection.
"It appears inflammatory cell death can be beneficial if it occurs in the early phase of infection," said co-first author Rajendra Karki, Ph.D., St. Jude Department of Immunology. "However, once the infection is established, the ZBP1-mediated PANoptosis inflammatory cell death mechanism promoted by interferon therapy becomes detrimental by resulting in cytokine storm, inducing tissue damage, morbidity and mortality."
These results have important implications not only for COVID-19, but also for potential therapies for other infectious and inflammatory diseases where interferons drive pathology.