Heliobas Disciple
TB Fanatic

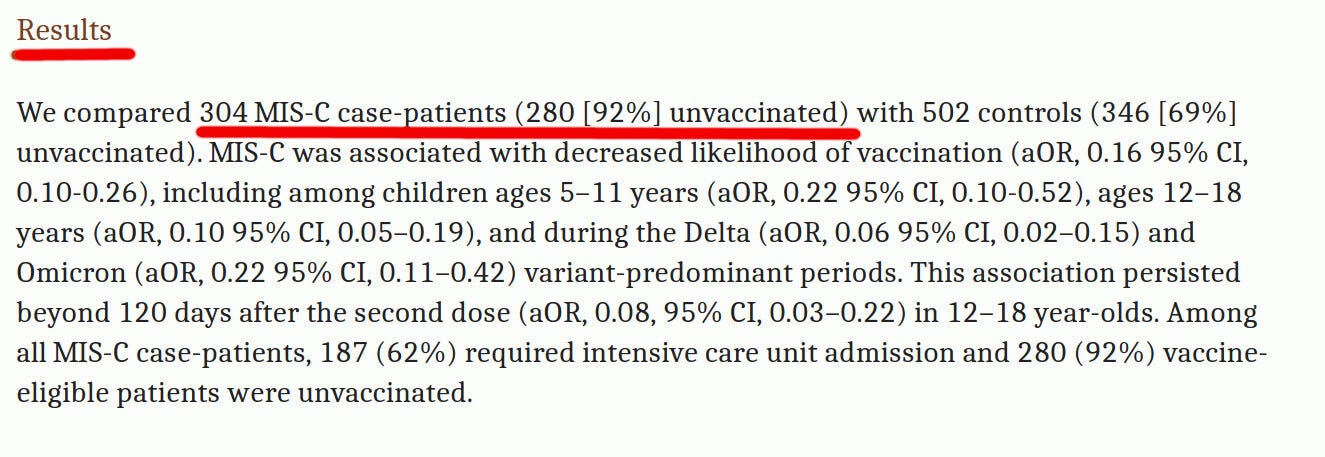
‘Stunning’: The Real Reason Health Officials Won’t Let Independent Scientists Examine mRNA Vaccine Vials
A data leak suggests the real reason health officials don’t want individual vaccine vials examined by independent scientists is that the vials are all different — and the mRNA in the shots is not intact.
 childrenshealthdefense.org
childrenshealthdefense.org
‘Stunning’: The Real Reason Health Officials Won’t Let Independent Scientists Examine mRNA Vaccine Vials
A data leak suggests the real reason health officials don’t want individual vaccine vials examined by independent scientists is that the vials are all different — and the mRNA in the shots is not intact.
By Dr. Joseph Mercola
09/13/22
Story at a glance:
- The reason health officials don’t want individual vaccine vials examined by independent scientists is that the vials are all different — and the mRNA in the shots is not intact.
- For an effective mRNA product, the mRNA integrity needs to be 100%, meaning all the RNA must be intact. Considering how ineffective the jabs are, it seems fair to question whether lack of mRNA integrity might be to blame.
- Fragmented RNA could potentially also be hazardous to health by generating incomplete spike proteins. While we do not know if incomplete spike proteins are dangerous, it’s possible they might contribute to cellular stress.
- The “bad batch” phenomenon may also be indicative of quality problems. Independent investigations have revealed that some lots of the shots are associated with very severe side effects and death, whereas other lots have very few or no adverse events associated with their use.
- However, the fact that “hot” lots are being released in a coordinated fashion suggests vaccine makers may in fact be doing intentional lethal-dose testing on the public, and that these “bad batches” are not merely the result of intermittently poor manufacturing.
A 14-minute video (below) that has been overlooked for nearly two years has now resurfaced, exposing stunning information about the COVID-19 jabs and why health officials don’t want individual vaccine vials examined by independent scientists.
What does the EMA leak show?
This video, and it's contents, are published on the grounds of public interest and public safety. The contents disclosed were the minimum necessary to back-up my claims. As neither Pfizer nor the European Medicines Agency will confirm the leaked information, their veracity is unknown, however...
The reason, it turns out, is because the vials are all different — and the mRNA in the shots “is not intact.” Both of these pose potentially serious problems.
In an Aug. 31 Substack article, Steve Kirsch explains:
“Even if you are getting 100% intact mRNA which would be really rare, you’re still not getting anything that resembles the virus. So the efficacy as far as PROTECTING you will be next to nothing.
“However, what it will do very effectively, if you got reasonably intact mRNA, is to cause you significant harm. You are playing a game of chance with your immune system and what is in the bottle.”
The video notes that members of the European Parliament were only allowed to read the contracts with the drug makers after they’d been heavily redacted. Why the heavy-handed secrecy, even toward legislators?
Leaked documents reveal serious quality issues
The finding that the mRNA in the shots was of questionable quality was revealed in a British Medical Journal feature investigation article published in March 2021.
As explained by the author, journalist Serena Tinari, cyber attackers retrieved more than 40 megabytes of Pfizer COVID-19 jab data from the European Medicines Agency (EMA) in December 2020.
The hacked data was subsequently sent to journalists and academics worldwide. It was also published on the dark web. Some of the documents show European regulators had significant concerns over the lack of intact mRNA in the commercial batches sampled.
Compared to the clinical batches, i.e., the shots used in the clinical trial, 55% to 78% of the commercial shots had “a significant difference in % RNA integrity/truncated species.”
In one email, dated Nov. 23, 2020, a high-ranking EMA official noted that the commercial batches failed to meet expected specifications, and that the implications of this RNA integrity loss were unclear. In response to the findings, the EMA sent a list of questions and concerns to Pfizer.
While we do not know if and how the EMA’s concerns were actually addressed and corrected, the EMA authorized Pfizer’s COVID-19 jab Dec. 21, 2020.
According to its public assessment report, “the quality of this medicinal product, submitted in the emergency context of the current (COVID-19) pandemic, is considered to be sufficiently consistent and acceptable.”
Similarly, Health Canada told the Britsh Medical Journal that “changes were made in their processes to ensure that the integrity was improved and brought in line with what was seen for clinical trial batches.” The EMA further tried to deflect concern by claiming some of the leaked documents had been doctored.
As reported by the British Medical Journal:
“EMA says the leaked information was partially doctored, explaining in a statement that ‘whilst individual emails are authentic, data from different users were selected and aggregated, screenshots from multiple folders and mailboxes have been created, and additional titles were added by the perpetrators.’”
Intact mRNA is essential to its effectiveness
Curiously, when the Britsh Medical Journal asked Pfizer, Moderna, CureVac and several regulators to specify the percentage of mRNA integrity considered acceptable, none replied with specifics.
According to the British Medicines and Healthcare Products Regulatory Agency, the FDA and Health Canada, the specification limit on RNA integrity is “commercially confidential.” What we do know — and the EMA has acknowledged — is that intact mRNA is essential for efficacy.
As noted by the Britsh Medical Journal:
“The documents offer the broader medical community a chance to reflect on the complexities of quality assurance for novel mRNA vaccines, which include everything from the quantification and integrity of mRNA and carrier lipids to measuring the distribution of particle sizes and encapsulation efficiency.
“Of particular concern is RNA instability, one of the most important variables relevant to all mRNA vaccines that has thus far received scant attention in the clinical community. …
“RNA instability is one of the biggest hurdles for researchers developing nucleic acid based vaccines. It is the primary reason for the technology’s stringent cold chain requirements and has been addressed by encapsulating the mRNA in lipid nanoparticles.
“‘The complete, intact mRNA molecule is essential to its potency as a vaccine,’ professor of biopharmaceutics Daan J.A. Crommelin and colleagues wrote in a review article in The Journal of Pharmaceutical Sciences late last year.
“‘Even a minor degradation reaction, anywhere along a mRNA strand, can severely slow or stop proper translation performance of that strand and thus result in the incomplete expression of the target antigen.’”
For an effective product, mRNA integrity needs to be 100%. Considering how ineffective the jabs are, it seems fair to question whether lack of mRNA integrity might be to blame. We also do not know whether nonintact mRNA might be harmful.
As noted by Kirsch, “Unstable mRNA means the spike protein … could collapse, making the whole process useless to support immunity, but still dangerous in terms of damage to cells. So, you get all the risk and no benefit.”
While our public health agencies claim fragmented RNA poses no health risk, just how do they know that? The leaked documents revealed they specifically did not have an answer to that question, and no research into the matter has been published, that I’m aware of.
Fragmented RNA may produce incomplete spike proteins
In May 2021, Stephanie Seneff, Ph.D., a senior research scientist at MIT for over five decades, published an excellent paper in which she highlighted several potential dangers of the COVID-19 jabs, including the unknown hazard of injecting fragmented RNA.
That same month, I interviewed her about her concerns. You can find that interview in “COVID Vaccines May Bring Avalanche of Neurological Disease.”
In her paper, Seneff noted:
“The EMA Public Assessment Report … describes in detail a review of the [Pfizer] manufacturing process … One concerning revelation is the presence of ‘fragmented species’ of RNA in the injection solution.
“These are RNA fragments resulting from early termination of the process of transcription from the DNA template.
“These fragments, if translated by the cell following injection, would generate incomplete spike proteins, again resulting in altered and unpredictable three-dimensional structure and a physiological impact that is at best neutral and at worst detrimental to cellular functioning.
“There were considerably more of these fragmented forms of RNA found in the commercially manufactured products than in the products used in clinical trials. The latter were produced via a much more tightly controlled manufacturing process. …
“While we are not asserting that non-spike proteins generated from fragmented RNA would be misfolded or otherwise pathological, we believe they would at least contribute to the cellular stress that promotes prion-associated conformational changes in the spike protein that is present.”
Kirsch points out that the EMA also expressed concern over visible particles in the vials, which the Britsh Medical Journal did not follow up on. “Is it still a problem?” Kirsch asks. That’s a good question, and the answer is probably yes.
But even worse is that we have absolutely no idea what these incomplete spike proteins are doing, none, zero, nada. It has never been directly examined. For that matter efforts to evaluate, and complications of the jab, have been consciously suppressed as have following simple metrics such as increases in all-cause mortality.
Deaths dismissed and side effects misclassified
The leaked EMA documents also showed that Pfizer dismissed all deaths in its trial as “unrelated to the vaccine,” even though no proper investigation was ever conducted.
We now have additional evidence of this — just like the court-ordered FOIA documents showed what Pfizer did in their U.S. trials. At least they are consistent in implementing their fraud.
As reported by Children’s Health Defense (CHD) back in June, Freedom of Information Act (FOIA) documents, released by court order, reveal Pfizer classified nearly all severe reactions in its trials as unrelated to the shot, even in cases where the health problems in question are extremely difficult to dismiss as anything other than a direct effect of the shot:
“The latest release by the U.S. Food and Drug Administration (FDA) of Pfizer-BioNTech COVID-19 vaccine documents reveals numerous instances of participants who sustained severe adverse events during Phase 3 trials. Some of these participants withdrew from the trials, some were dropped and some died. …
“The CRFs [case report forms] included in this month’s documents contain often vague explanations of the specific symptoms experienced by the trial participants. They also reveal a trend of classifying almost all adverse events — and in particular severe adverse events (SAEs) — as being ‘not related’ to the vaccine. …
“The many serious adverse events — and several deaths — recorded during the Phase 3 trials are also apparent in a separate, massive document exceeding 2,500 pages, cataloging such adverse events.
“This document lists a wide range of adverse events suffered by trial participants classified as toxicity level 4 — the highest and most serious such level. However, not one of the level 4 (most severe) adverse events listed in this particular document is classified as being related to the vaccination.”
As just one example, a teenage girl got the shot Sept. 11, 2020, and in mid-November 2020 was diagnosed with right lower extremity deep vein thrombosis, which we now know is a potential side effect of the jab.
According to the CRF, her condition was due to a bone fracture that occurred before the date of her injection — a determination that seems questionable at best.
What’s the cause behind the ‘bad batch’ phenomenon?
The “bad batch” phenomenon may also be indicative of quality problems. Independent investigations have revealed that some lots of the shots are associated with very severe side effects and death, whereas other lots have very few or no adverse events associated with their use.
According to howbadismybatch.com, a site that matches up vaccine lot codes with reports in the VAERS system, approximately 5% of the lots are responsible for 90% of all adverse reactions. Some of these batches have 50 times the number of deaths and disabilities associated with them, compared to other lots.
Another website that basically does the same thing is WelcomeTheEagle’s VAERS Dashboard. A video explaining how to use the dashboard can be found on Bitchute.
However, an even deeper dive into this data suggests random quality issues are not the problem. In the video above, Reiner Fuellmich, cofounder of the German Corona Investigative Committee, and Dr. Wolfgang Wodarg, a former member of the German parliament, discuss this “smoking gun” evidence.
According to Fuellmich and Wodarg, the lot-dependent data suggests vaccine makers may be conducting secret experiments within the larger public trial. In other words, they appear to be doing lethal-dose testing on the public.
The tipoff that these “hot” batches are not caused by intermittent poor manufacturing is the fact that they’re being released in a coordinated fashion.
Wodarg argues that the evidence for this is very clear from the data. Basically, the vaccine manufacturers are coordinating their lethal-dose experiments so that they’re not all releasing their most toxic lots at the same time, or in the same areas. This avoids detection through clustering.
New boosters will not undergo additional testing
Considering the multitude of open questions surrounding the safety of the original COVID-19 shots, the fact that new, reformulated boosters will not require any additional testing whatsoever is beyond disturbing.
In the “Friday Roundtable” video above, Dr. Meryl Nass, Toby Rogers, Ph.D., Aimee Villella McBride, Polly Tommey and Brian Hooker, Ph.D., discuss the FDA’s decision to allow vaccine makers to reformulate their COVID-19 shots without additional testing, in perpetuity.
As noted by Rogers, Pfizer’s bivalent booster against Omicron variants BA.4 and BA.5 was tested on a total of eight mice, and only to check antibody levels. Moderna also used mice to ascertain antibody responses, but has not disclosed the number of mice used.
That’s the extent to which these shots were tested. The original COVID-19 jabs are the most dangerous drugs ever released to the public, and these newer boosters may turn out to be even worse.
As explained by Rogers, the shots “imprint” your immune system to respond only to the antigen in the shot, while simultaneously impairing your immune system so that it’s less capable of protecting you against other pathogens.
Another term for this process is “original antigenic sin.” It essentially explains why those who are jabbed are getting infected and sicker than those who avoided the jabs.
Rogers predicts we’ll be faced with a winter of severe illness and death among those who have gotten the jabs. All the rest of us can do is stand back, avoid the shots at all costs and “let the mainstream system self-destruct.” Hopefully, he’s correct in his other prediction, which is that the vast majority of Americans will reject these boosters.