because it would certainly fit as part of a larger pattern

boriquagato.substack.com
(fair use applies)
is pfizer suppressing vaccine adverse events reports in infants?
because it would certainly fit as part of a larger pattern
el gato malo
15 hr ago
the legacy US press has become a sad and captured thing that desperately cheer leads for such advertisers as remain to fund the melting iceberg of its former glory as it drifts off into irrelevance.
but this is not so in some of the rest of the world and this is why reading foreign news is often the best way to learn what’s actually happening in america. this goes double for foreign policy and squintuplety-zillion (possibly not a real number) times for anything touching pharma because pharma advertising is the backbone of american media and you criticize the golden goose at your bottom line’s existential peril.
and this takes us to israel
whose press has been quite a lot freer and franker than our own on issues of covid vaccines.

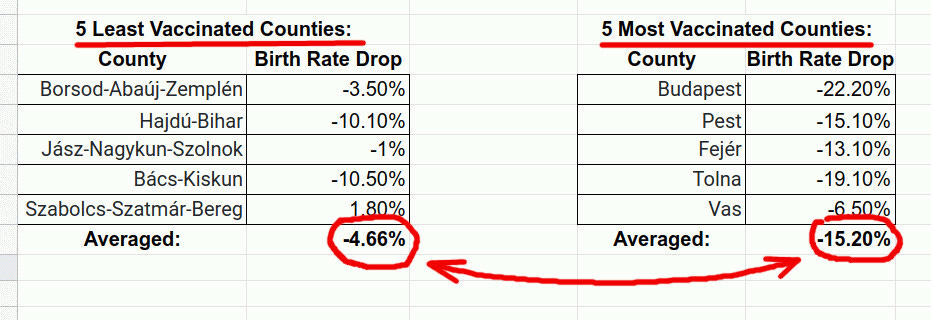
read the whole article, it’s terrifying. (and has some great data tables)
it describes a case of cardiac arrest in a previously healthy 2 month old male approx 1 hour after vaccination.
“Patient administered vaccination, observed for 15 minutes left the clinic then returned one hour later on 02 Feb 2021, presenting as skin cold, clammy and with chest pain, cardiac arrest event then developed, patient stabilised and transferred for further medical treatment… The outcome of the events was unknown. This case was reported as serious with seriousness criteria-life threatening from HA. No follow-up attempts possible. No further information expected".
Unsure if patient was enrolled in clinical trial”. However, the author of the report also states that the report was ”received from a contactable Other Health Care Professional by Pfizer from the Regulatory Agency”. This note implies that the infant might have actually participated in Pfizer's trial. The regulatory agency report Safety Report Unique Identifier GB-MHRA-ADR 24687611 - indicates that the report came from Great Britain (the first 2 letters in the report ID stand for the country of origin, GB- Great Britain, and MHRA indicate that the source of reporting was its' drug authority).
so, what exactly happened with this child?
- there is no other legal means to have dosed the child. if this were not in a trial, it would have been contra indicated, immoral, and likely illegal.
- the report appears to be from a pfizer associated HCP
this points to trial inclusion or at least pfizer involvement, but we do not know for sure and 2 months should be too young even for the most recent trial, so what exactly happened here is a bit of a puzzler.
and how did the child do? did they recover? we have no idea.
“
No follow-up attempts possible. No further information expected."
what on earth is that? i flat out cannot imagine any even half reasonable explanation to drop this child from follow up apart from the sinister one: that they did not want to know and so they are memory holing a baby who had a heart attack from their product.
this is already deeply worrying and indicative of possible manipulation and fraud.
but it gets MUCH worse.
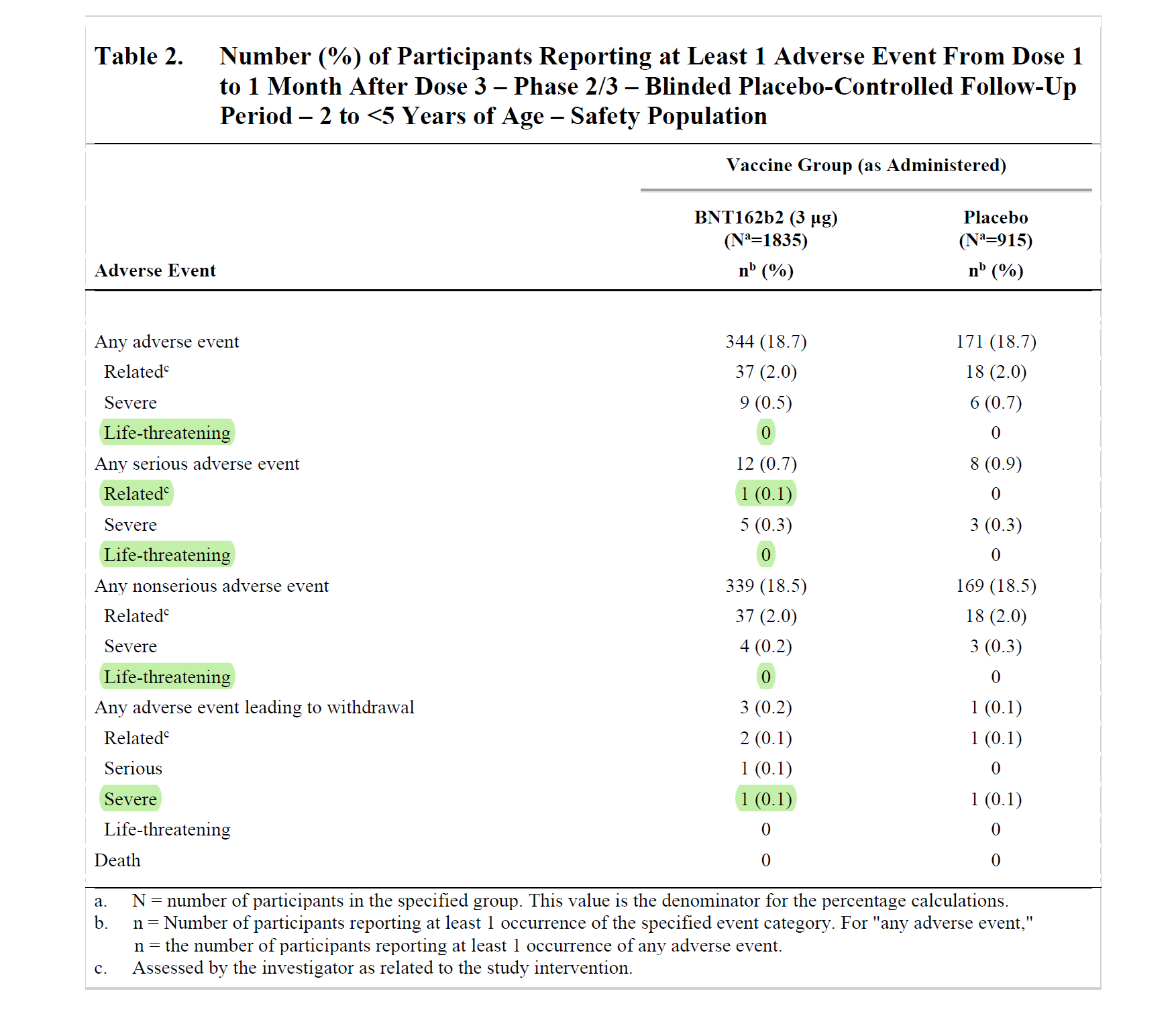
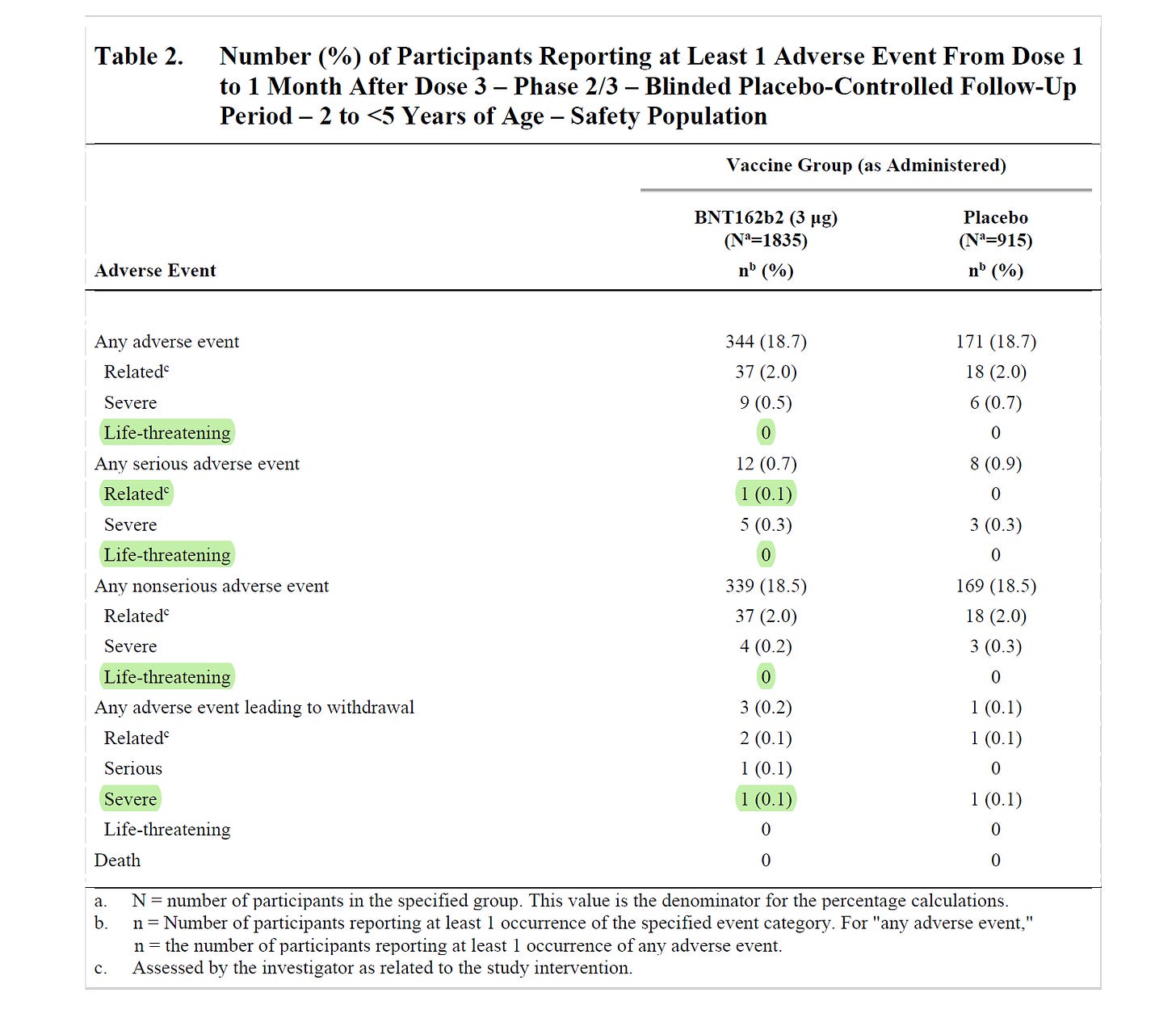
there was not a single life threatening event recorded in the entire pediatric trial. not one.
there was only one “related” severe event (out of 5 serious events, 4 of which were deemed “unrelated”)
(
SOURCE)
so, if this child was in the trial we’re already getting into some serious questions:
this sure looks to me like it ought to have been classified as life threatening. it’s cardiac arrest in a 2 month old.
but even if we’re going to call it “severe” instead, then this was it. the only related one in the whole trial.
and THAT is where we start to run into serious problems.
because this child was not an isolated case.
there were 58 of these. (and VAERS likely under-reports by 10-100X)
The analysis shows there were at least 58 cases of severe and life-threatening adverse reactions among babies and toddlers 3 years old and younger. This finding is especially puzzling considering the fact that they weren’t supposed to be vaccinated at this age to begin with. Sadly, similarly to the case reported above, most VAERS reports do not indicate how and under which circumstances they were exposed to the vaccine – were they participants in the companies' trials? And if not, why and in which circumstances were they vaccinated?
and if even one of these life threatening events was actually in the trial, we need to be asking some serious questions about fraud.
and it keeps getting worse.
many children in the VAERS reporting had massive responses with multiple effects.
and then they seem to have had no or conflicting follow up.
and they seem to be nowhere in the trial results.
these numbers are terrifying and if all were in the trial would imply an over 1% life threatening AE rate. that’s easily 100X the risk of covid to this group, probably more like 1,000 or even 10,000X.
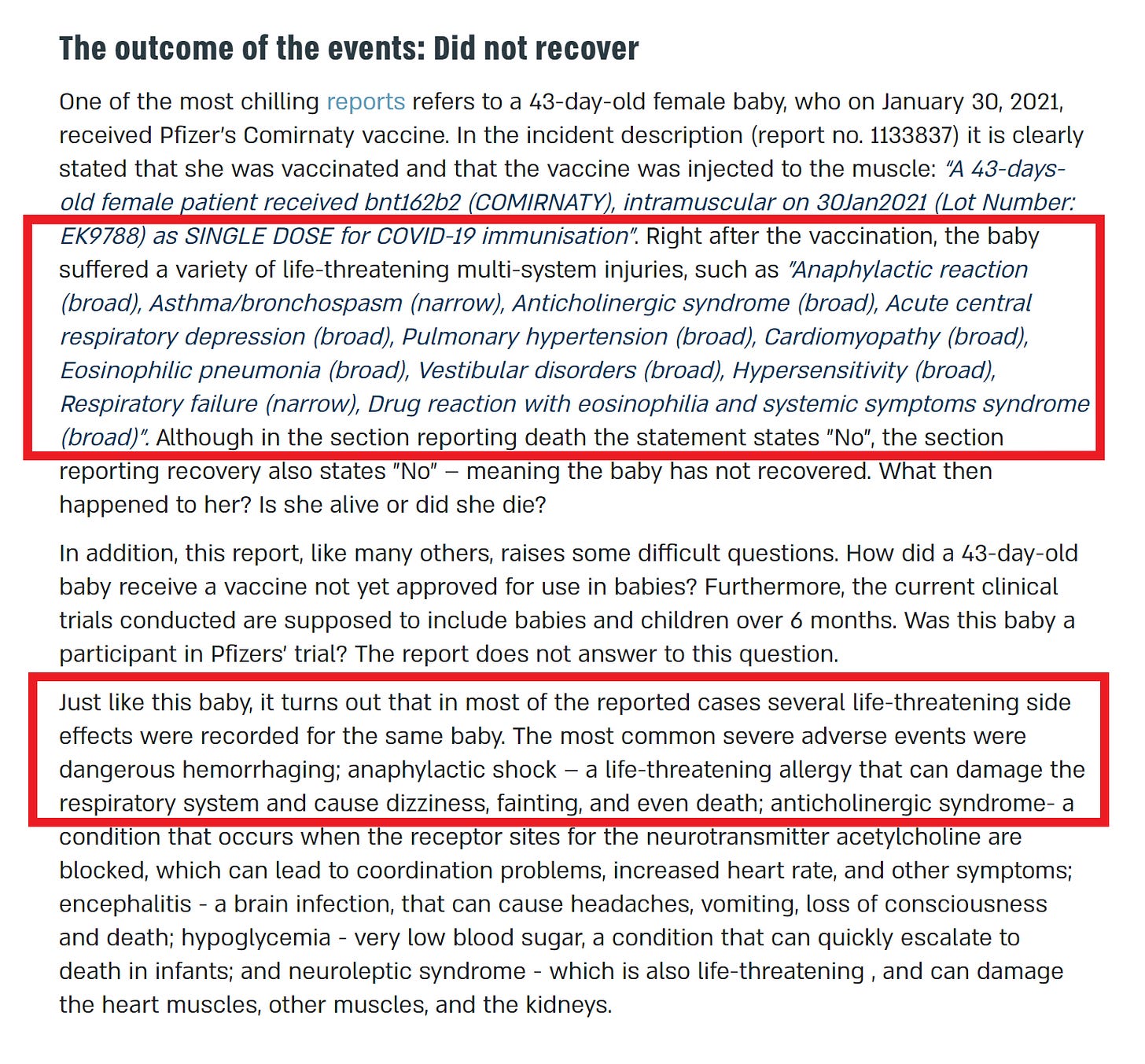
this is not subtle stuff. this is incredibly severe and systemic reaction. and the data is an obvious mess with children being described both as “not having recovered” but also “not having died” and disappearing like peter pan’s playmates.
this is screaming for investigation.
either many doctors all over the world are badly injuring babies by experimentally jabbing them with unapproved product (and i doubt this as lawsuits would be rife) or this was all part of the pfizer trial and they suppressed it.
place your bets.
pfizer have been playing outlandish games with their vaccine trials.
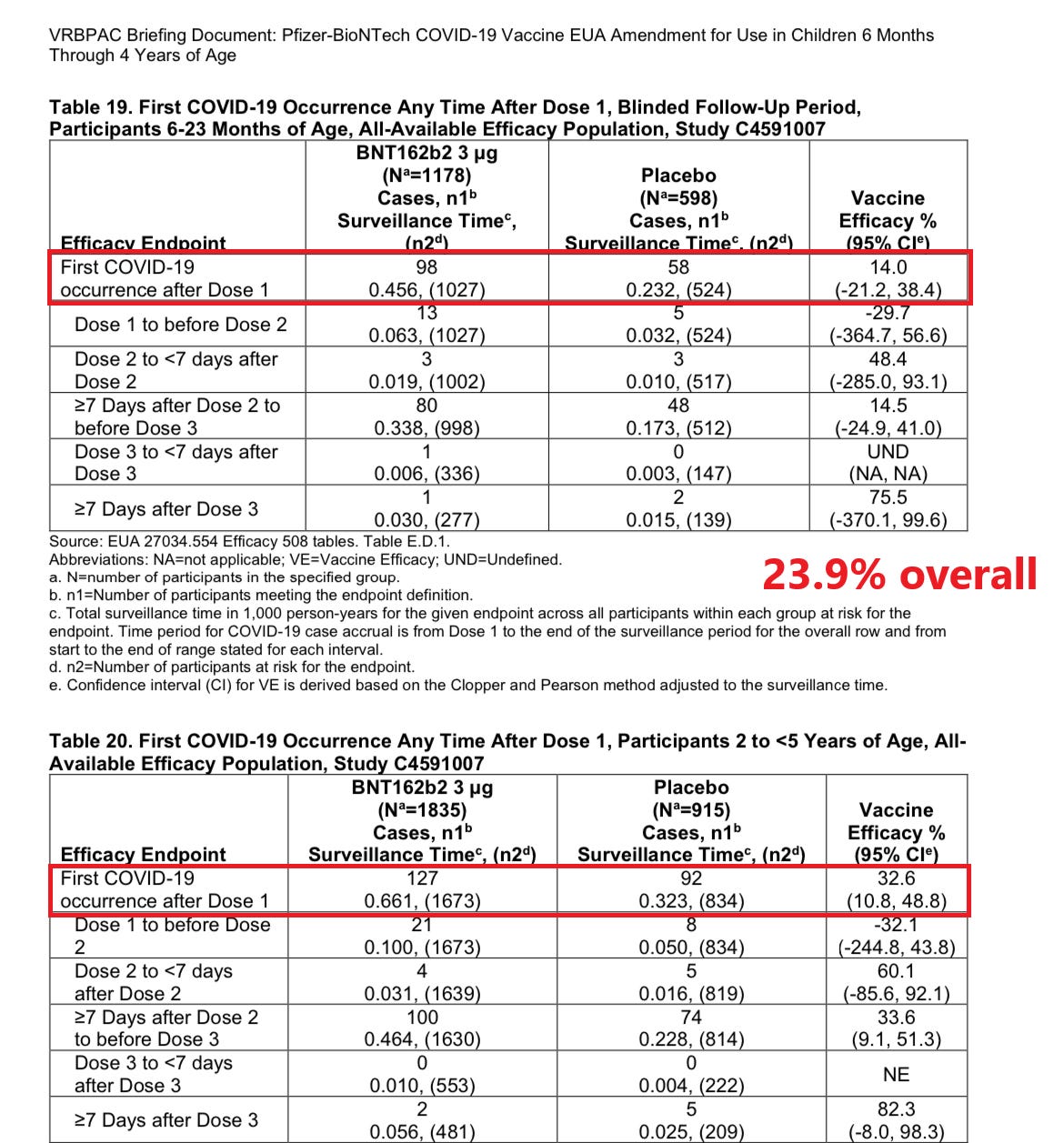
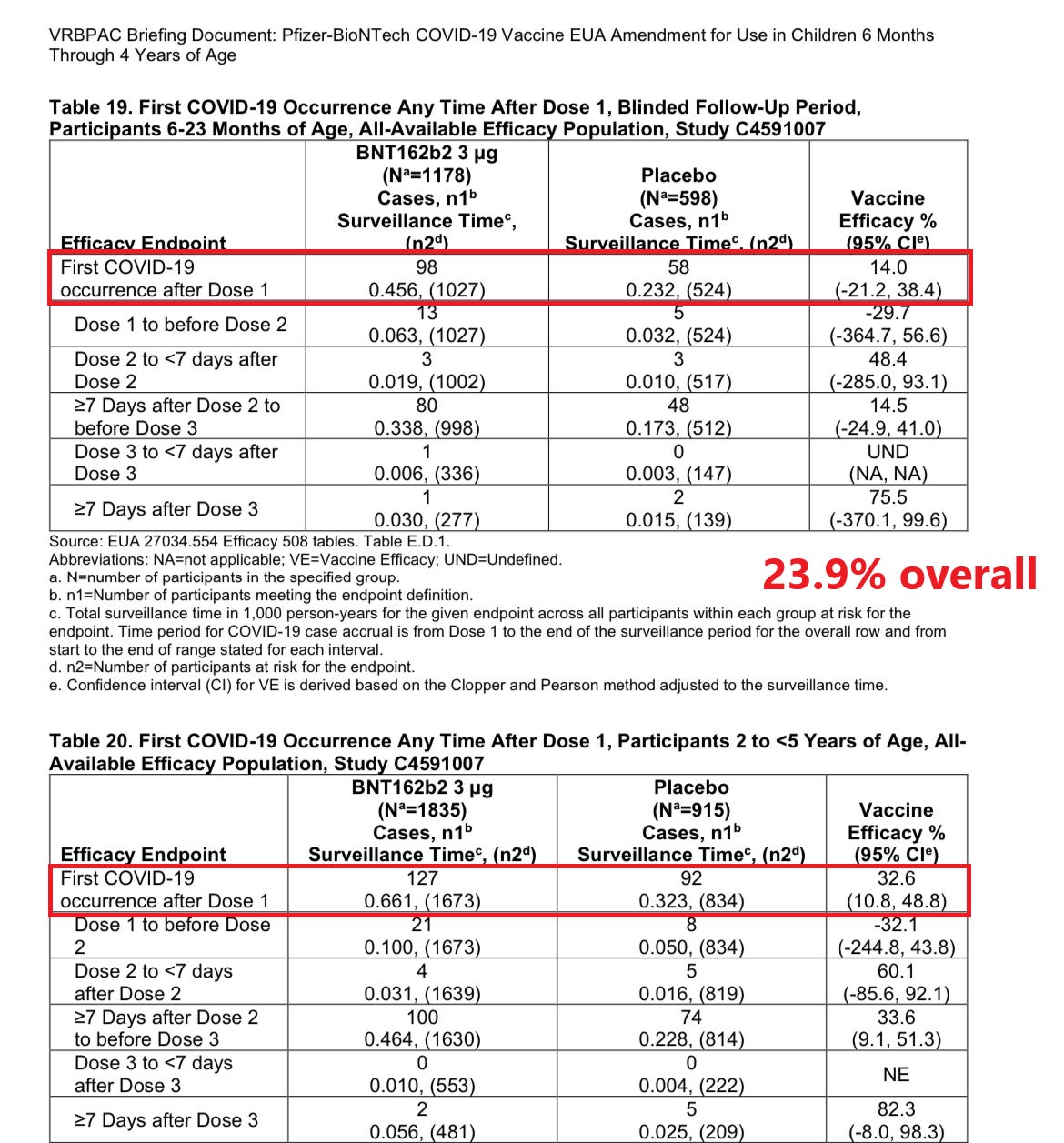
and the pediatric trial looks little different. their headline efficacy figures were the same bad methodology used to hide immune suppression all along. their headline result ignored a staggering 97% of cases in the trial by only counting from dose 3 + 7 days. real VE was 23%, not 80% and missed stat sig entirely in under 2’s.
they buried it in a supplement.
these are the sort of people we’re being asked to trust.
and the further one goes back into pfizer history, the less trustworthy they look. CEO albert bourla has a past so dark that if he applied for a position as a demon, asmodeus would probably pass him over out of fear of losing his job once alberto got settled in.
as so consistently seems to be the modal outcome, regulators were either asleep or captured.
pfizer is just about if not the most fined and sued pharma company in the world for a reason and the reason is “their behavior.”
their cattle vaccine (PregSure BVD) was causing massive, wholesale death in calves that nursed from mothers that got jabbed. the inoculant was given over and over as regular doses. the problems emerged, the data was clear, and pfizer fought it all.
they lied and denied and most of all kept selling and marketing the vaccine.
they claimed the side effects were overstated and unlinked.
calves were literally bleeding out through their eyes and ears and having “blood sweats.” it destroyed their bone marrow.
it was killing 15% of the junior moo team at some farms. this was not “long ago.” this was 2006. no one pulled it until 2010.
despite it being
well studied and established, my understanding is that pfizer denies the issues to this day.
the head of the animal division that did this was albert bourla.
albert is currently the CEO of pfizer.
they not only failed to fire him over this, they promoted him.
draw your own conclusions about their priorities from that…
big pharma is not like other pharma. i love small pharma. i know 100’s of wonderful people there, clever researchers and good eggs who are really, truly trying to figure things out and make good products.
but big pharma is not mostly development. they buy that. they are mostly marketing and sales and the best way to do that is regulatory capture and market domination. they play on a much bigger scale and those are they kinds of stakes that bring out the worst in people. those are the kind of stakes where you cannot admit you were wrong and it’s better to lie and keep killing people than allow mistakes to be known.
and this is far from isolated and far from new.
when you spend this kind of capital, both monetary and reputational, the gloves are off. you play dirty. you play to win. big pharma has a practices list that make big tobacco look like your neighborhood farm to table co-op.
it has ALWAYS been like this.

one of the things that’s been so surreally bizarre to me throughout all this branch covidian cultism is the radical society scale amnesia and inversion here.
3 years ago, everyone knew big pharma were nasty, self-serving, dishonest, rapacious entities. this was triple true on the left. and now they are the darlings and the saviors, they who must be trusted, they to whom we must defer. cuz, science.
this is like watching baby mice demanding to be babysat by malayan pit vipers.
it has to rank among the greatest marketing campaigns in human history.
they have not only rehabilitated their deservedly tarnished reputations but burnished them to a gleaming shine.
warp speed warped minds.
mordred has become sir gallahad.
we have forgotten who they are.
there is simply far too much smoke here to be no fire and i suspect that uncovering adverse event suppression is how this whole tawdry mess unravels.
people can forgive a failure to be effective. lots of drugs that barely or don’t work still sell well.
but they will not forgive being attacked, and that’s what suppressing reports of harms and side effects does.
they will especially not forgive an attack on their children.
and it’s failing. uptake is incredibly low, parents deeply suspect. skepticism is high and rising. and a real fight is brewing.
this was the bridge too far and with efficacy collapsed and outright inverted on infection, harms soaring and likely worse for boosters than originals, and the FDA doing nothing but tearing out all the safeguards and trying to make these jabs evergreen without clinical trials (like flu shots) it’s just getting too big to hide.
this will all come apart, collapsed under its own dead weight and declaring “fraud” will likely invalidate the EUA liability shields.
the world is going to turn on pfizer because it will be the low energy path and a way for the politicians who pushed this to play the victim and divert your anger.
europe is already waking up and post election, i suspect the US dominoes will start to fall as well.
“who knew what and when did they know it?” is going to become the name of the game.
the next 6-12 months are going to get pretty wild.
.



 www.theepochtimes.com
www.theepochtimes.com



 brownstone.org
brownstone.org
 jackanapes.substack.com
jackanapes.substack.com



 igorchudov.substack.com
igorchudov.substack.com


 alexberenson.substack.com
alexberenson.substack.com

 www.nature.com
www.nature.com







 markcrispinmiller.substack.com
markcrispinmiller.substack.com
 jessicar.substack.com
jessicar.substack.com