There will be blood
Election Day: Eight episodes that awakened parents to liberal indoctrination in schools
School trip to a gay bar, male student in skirt assaults girl in female bathroom, and a student sent to "the black class."justthenews.com
Election Day: Eight episodes that awakened parents to liberal indoctrination in schools
School trip to a gay bar, male student in skirt assaults girl in female bathroom, and a student sent to "the black class."
Updated: November 2, 2021 - 12:02am
From the marquee Virginia governor's contest to school board contests across America's suburbs, parents of schoolchildren are expected to play an outsized role in Tuesday's off-year election and provide a measurement of just how potent an issue liberal indoctrination in the U.S. education system has become to a restless electorate.
The unexpected rise of the school curriculum movement was sparked by a pandemic that trapped students at home with parents for months, unmasking what was being taught in classrooms and how it was being taught.
Parents suddenly become incensed that their children were being forced to conform to transgender-friendly language or subscribe to the notion the color of their skin was predetermining their future in an inherently racist America. Soon a revolt was waged, with parents confronting their educators and their school boards about such concepts as critical race theory and equity learning.
Along the way, stunning revelations cemented the determination that change was needed, from proclamations that parents don't deserve a say in what is being taught to schoolchildren to disclosures that highly sexualized books involving abortion and pedophilia were being assigned to young students.
"I was able to see into the classroom and see what was being taught and how it was being taught," explains Lysa Kosins, one of three of moms who banded together in a bid Tuesday to oust long-term school board members in the Dayton, Ohio, suburb of Centerville. "And you know, it doesn't work. We need to start treating our kids like individuals, and we need to start allowing the parents who really know what is in the best interest of our children to make choices that better fit their educational needs."
Here are eight defining moments that catapulted the fight against liberal school indoctrination into a nationwide movement that has sparked more than 80 school board recall elections this year.
The wealthy enclave in Loudoun County, Va., became ground zero for the parents' rights movement this past spring, as its school board pushed through equity learning and gender neutrality provisions over objections from parents who don't believe that students must be guaranteed equal outcomes or that teachers or students who don't comply with the gender identification wishes of transgender students should be punished.
- A Washington suburb's push for equity learning and gender neutrality ignites a protest.
Already in the midst of an intense parent revolt, Loudoun County emerged anew to the forefront of the debate this fall with revelations a biological male student wearing a skirt committed a sexual assault on high school girls in the female bathroom. The offender has been convicted of committing two unwanted sex acts on one girl and faces charges of a sex assault on another girl at a different school. Students have now launched their own protests over what they saw as a coverup.
- A coverup of skirt-wearing male student's sexual assault on a girl in a female bathroom.
A parents-led movement in the affluent community of Southlake became the national proof of concept in May, when candidates who renounced their school district's racial equity curriculum won every race by wide margins, including two school board seats, two city council seats and the mayor's office. Since then, more than 80 school board recall elections have been launched targeting more than 200 officeholders, more than triple a normal election year's tally, according to Ballotpedia.
- The election in Southlake, Texas, affirms parents have the electoral muscle.
In Virginia's closely watched gubernatorial race, Republican outsider Glenn Youngkin was already tapping into the suburban parents' angst over ideologically-infused education when his Democrat opponent, Terry McAuliffe, uttered an unforgettable line in their final debate, transforming the race. "I'm not going to let parents come into schools and actually take books out and make their own decision," McAuliffe declared. "... I don't think parents should be telling schools what they should teach." Almost instantly, the race changed in the reliably blue state to a dead heat in a political bellwether that swept across the country.
- Terry McAuliffe and the debate line heard around the country.
No single event had more impact in transforming the predominantly local debate over school curricula to a federal issue than Garland's ill-fated memo asking the FBI to investigate parents' threats against school board members, which was prompted by the National School Boards Association's letter equating parents with domestic terrorists. The association had to apologize, and Garland has spent weeks trying to explain his edict to distrustful members of Congress.
- Attorney General Merrick Garland unleashes the FBI on parent protests.
The reverberations were still being felt Monday, when Sen. Chuck Grassley (R-Iowa) renewed his request to have Garland retract his memo. "Mr. Attorney General, parents are not domestic terrorists, and you have only one reasonable choice," Grassley said from the Senate floor. "Withdraw your memo and focus on the real threats. Stop being a pawn for the White House by politicizing the Department of Justice."
A group of teachers in Springfield, Mo., opened a new front in the school curriculum battle when they filed suit saying they were subjected to illegal and discriminatory training videos centered around Critical Race Theory. Their suit accused the school district of violating their First Amendment rights by requiring them to take Critical Race Theory training, which included telling the employees to vote for socialist candidates
- Teachers in one Missouri school district fight back against training they deemed racist.
Kila Posey made national waves when she and her husband filed a complaint with the U.S. Department of Education's Office for Civil Rights over the local elementary school principal's segregation of classrooms, a submission that included recordings of their conversations with administrators. Posey alleged that when she tried to pick the classroom that was best for her daughter, who is black, her principal proclaimed, "That's not the black class." Their case prompted other complaints, including a lawsuit this month alleging similar racial segregation in a Massachusetts school district.
- 'That's not the black class.' An Atlanta mom stands up to racial segregation of classrooms.
When a Florida elementary school class in Broward County recently took its students to a gay bar and grill, there was bipartisan outrage over the choice of the venue. Some believed it was an effort by educators to introduce students to a gay lifestyle, while others found it inappropriate for kids to be in a drinking establishment.
- A class trip to a gay bar ignites disbelief.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
GOV/MIL Leftists Call For New "Secret Police" Force To Spy On Trump Supporters (AN ABSOLUTELY MUST-READ THREAD)
- Thread starter marsh
- Start date
-
- Tags
- gestapo secret police
marsh
On TB every waking moment
Neo-Marxism in the Military: Dr. Ron Scott and Lt. General Rod Bishop 51:26 min
Neo-Marxism in the Military: Dr. Ron Scott and Lt. General Rod Bishop
The Professor's Record with David K. Clements Published November 3, 2021
Critical Race Theory and Marxism running amok in the military? Yes sir.
Learn from these veterans on how they plan to fight back.
To find out more about the work of Col. Ron Scott and Lt. General Rod Bishop and STARRS, visit their website https://www.starrs.us/.
To find out more about Dennis Haugh visit The Current Constitutional Crises
Neo-Marxism in the Military: Dr. Ron Scott and Lt. General Rod Bishop
The Professor's Record with David K. Clements Published November 3, 2021
Critical Race Theory and Marxism running amok in the military? Yes sir.
Learn from these veterans on how they plan to fight back.
To find out more about the work of Col. Ron Scott and Lt. General Rod Bishop and STARRS, visit their website https://www.starrs.us/.
To find out more about Dennis Haugh visit The Current Constitutional Crises
marsh
On TB every waking moment

GOP: The Fight Against Critical Race Theory Has Only Just Begun
The GOP shows no signs of backing away from the fight to keep leftists from indoctrinating children in schools.
 www.breitbart.com
www.breitbart.com
GOP: The Fight Against Critical Race Theory Has Only Just Begun
 being taught in schools at the Loudoun County Government center in Leesburg, Virginia on June 12, 2021. - Are you ready to take back our schools? Republican activist Patti Menders shouted at a rally opposing anti-racism teaching that …")
KATHERINE HAMILTON3 Nov 202165
Republicans waded neck-deep into the culture war in the fight against Critical Race Theory and government overreach — a tactic that served them extremely well in the Virginia governor race on Tuesday.
Democrats and corporate media have largely reduced Governor-elect Glenn Youngkin’s win to a product of white supremacy instead of taking the opportunity to reflect and change their strategy moving into the midterms and into 2024. The GOP however, shows no signs of backing away from the fight to keep leftists from indoctrinating children in schools, especially if Democrats repeat the mistakes they made in the Virginia election by gaslighting voters on issues that directly impact Americans and their families.
Figures in the conservative and political realm reacted to Youngkin’s win on Twitter, seemingly conflating the victory in part with voters’ rejection of the leftist ideology.
Sen. Josh Hawley (R-MO) pointed to the Virginia election results as a sign “voters don’t want what the Democrats are selling.”:
The message from last night’s GOP sweep in VA and the shocker of a race NJ is crystal clear: voters don’t want what the Democrats are selling. They don’t want parents persecuted, they don’t want critical race theory, they don’t want woke liberalism.
The official House Republicans Twitter account also dissed the theory, noting that it is “NOT history” and citing a Fox News poll that found that Critical Race Theory was one of the top issues driving voters to the polls.

“The VA election is the beginning of a parents revolt about fighting Critical Race Theory (BLM), protecting our daughters and exposing the consequences of pushing radical gender ideology. Win or lose, moms and dads have had enough,” American Conservative Union Chair Matt Schlapp forecasted before Youngkin’s win.

Sen. Marsha Blackburn (R-TN) also chimed in, touting parents’ rejection of the Democrat agenda.
“Parents overwhelmingly reject critical race theory in their child’s education,” Blackburn said.
Democrats were already on shaky ground before the Virginia election. Infighting and a president with a spiraling approval rating on almost all key policy issues pose a threat to their control in the House and the Senate. Vice President Kama Harris herself said the outcome of the election would show “how the country is gonna move.”

“Don’t Texas Virginia,” Harris warned, “What happens in Virginia will, in large part, determine what happens in 2022, 2024, and on.”
marsh
On TB every waking moment
Microsoft employees say hello by pronouns and race…
This is so disturbing I thought it was fake, but these people check out as legit employees. A second video from Microsoft has surfaced.  …
 citizenfreepress.com
citizenfreepress.com
Microsoft employees say hello by pronouns and race…
Posted by Kane on November 4, 2021 2:14 pm
View: https://twitter.com/i/status/1456276894664384523
.23 min
This is so disturbing I thought it was fake, but these people check out as legit employees.
A second video from Microsoft has surfaced.
View: https://twitter.com/i/status/1456344147103653889
1:03 min
marsh
On TB every waking moment
.58 min
The DOJ Does Not Appear to Be Run by the Attorney General | Truth Over News
Premiered 2 hours ago

The Epoch Times
marsh
On TB every waking moment
marsh
On TB every waking moment


The Media Struggle Session Over Elections and Education Is Withering Under the Arrival of Facts
By Brad Slager | Nov 04, 2021 6:00 PM ET

Sit back and watch our media elites embarrassing themselves as they attempt to humiliate while ignoring facts.
Few things are as illuminating about the rigged system within our media complex as an election cycle. The coverage of the candidates and the favoritism displayed is one aspect, and then there are the results. There is a clear dichotomy on display depending on who wins; a Democrat being elected is a sign of a wise populace who has given free rein to the winner via a mandate. When a Republican wins they need to understand they narrowly achieved victory and still have to heed the voices of the disenfranchised.
There is one other difference. Democrats win and prove the uncritical perfection of our system, while a GOP win results in the press turning introspective and trying to figure out what went wrong. It is how we arrive at Donald Trump spending months denying he lost being called an open threat to democracy, while Stacey Abrams can live for years in abject denial of her election loss and become elevated in her party. The press tells us how they resent Democrat losses and immediately look for a fix.
Note how we are currently enduring long segments of game-film analysis and lengthy think pieces about the accursed racism of Tuesday’s winners. We never hear pundits delivering somber post-mortems on Republican defeats; we usually hear how the voters repudiated outmoded and intolerant policies and the GOP needs to get with the times. But give them a Republican show of strength and there is a problem, and as a result, the journalists have tied themselves into knots this week.
The first issue is both the most obvious, and the laziest — Republicans campaigned on fear and motivated their racist base. This has led to the hilarious conclusion that in Virginia, a black lieutenant governor and a Hispanic attorney general winning for the first time ever proves Republicans are racist because they did not elect the nearly translucent image of political privilege, Terry McAuliffe.
But what has the media dizzy in confusion is how the Republicans won on messaging regarding schools, the topic thought to be owned by Democrats.
School boards acting authoritarian, parents being told to pipe down and shut up, and Terry McAuliffe telling them they had no say in the education of their own children created a fierce backlash. This is obvious to many of us, but the deeply intelligent thinkers in the press are struggling with this.
At the New York Times, they attempt to get their arms around this issue but become tripped up by their entrenched bias. They telegraphed their problems in just their headline, resorting to the tired explanation of “Republicans Pounce,” before changing it out not once but twice.


But to listen to these geniuses try to explain what happened you get the distinctive tang of resentment in the explanation. It is as if the candidates were just throwing stuff out there, hoping for something to take root, and managed to get just lucky enough that something latched on in the minds of enough bewildered voters.
Since they are really grappling with finding the cause of things here, allow me to futilely attempt to explain it for them. From the start of the pandemic lockdowns, conservatives have criticized the governmental overreach, and when it came to the school closures, and then teachers unions in some states holding the reopening of schools hostage it was criticized even more. The candidates arriving are fighting those exact same battles.Seizing on education as a newly potent wedge issue, Republicans have moved to galvanize crucial groups of voters around what the party calls “parental rights” issues in public schools, a hodgepodge of conservative causes ranging from eradicating mask mandates to demanding changes to the way children are taught about racism. Yet it is the free-floating sense of rage from parents, many of whom felt abandoned by the government during the worst months of the pandemic, that arose from the off-year elections as one of the most powerful drivers for Republican candidates.
It does not concern “what the party calls parental rights,” it is their actual rights as parents. Here you have New York Times reporters that cannot even entertain the concept that parents have the authority to make decisions regarding their own child. Then calling the issues a “hodgepodge” only illustrates the lack of curiosity they had in exploring things. Whether it was the curriculum, school closings, mask mandates — all of it tied into the school boards and teachers’ unions exerting too much control over the wishes of parents.
The denial in this piece is grand because at first, they take great pains to lay out how this is all contrived outrage. They claim that Republicans sensed an opening, “While the conservative news media and Republican candidates stirred the stew of anxieties and racial resentments that animate the party’s base,” in order to get a political foothold with voters. But then, very deep in the article, do they only begin to reveal some fundamental realities.
Just look at what is on display here. After about 800 words spent demonizing the allegedly scattershot and racist-driven agenda of the Republicans, they admit to them addressing directly the issues which concerned parents, and those being from a number of minority groups. The Times writers first claim this was all a cooked-up hysteria by the party and right-wing outlets, but then admit they were addressing legitimate concerns felt by those all across the political spectrum.But the election results suggested that Republicans had spoken about education in ways that resonated with a broader cross-section of voters. In Virginia, the Youngkin campaign appealed to Asian parents worried about progressive efforts to make admissions processes in gifted programs less restrictive; Black parents upset over the opposition of teachers’ unions to charter schools; and suburban mothers of all races who were generally on edge about having to juggle so much at home over the last year and a half.
This bifurcated wisdom is seen elsewhere in the press. After Tuesday’s results, Critical Race Theory is all the focus, with the press desperately trying to reclassify what it is — or even if it exists. You see countless pundits making the blatantly false claim that it is not even being taught in schools. It is a lie, and it is one I will be addressing in an upcoming piece. But just look at the paradox the journalists have created for themselves.
So flustered are they by this repudiation of CRT that inspired parents from various demographics to oppose it, many in the press are trying to deny its very existence.
Nicolle Wallace:
View: https://twitter.com/i/status/1455693642866298887
.48 min
Andrea Mitchell:
View: https://twitter.com/i/status/1455722970668806148
.57 min
So, a question, you galaxy brains–
How can Republicans/right-wing media/parents be racist for blocking something that does not exist? If CRT is not real, and/or this whole issue is a contrivance — a conspiracy theory over non-existent content — why is it such a hot-button issue that it has caused people to move across party lines to fight it? This would have been stopped from day-1 by simply illustrating that it is not anything tangible.
Then we are back to that devilish five-letter word — proof. We know it exists, we have seen the documents and heard the lobbying on behalf of installing the curriculum. If this was a phantom issue there is no way it would be fought over this long, and up to today.
Plus you cannot tell parents they are racists for trying to prevent something from being taught in schools if the thing that makes them a racist also does not exist. It would be like alleging Jim Crow laws exist today because businesses are banishing your imaginary friend from using a particular water fountain. And this underscores so much of the problem we see in the press today — they refuse to make friends with reality.
marsh
On TB every waking moment
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
 www.zerohedge.com
www.zerohedge.com
California's Attempt To Hobble Gifted Students Over 'Racial Disparities' Starting To Backfire
BY TYLER DURDEN
SATURDAY, NOV 06, 2021 - 10:30 PM
California's attempts to eliminate accelerated math courses for gifted students was a terrible idea from the beginning. Now it's beginning to backfire.
Critics of the draft said the authors were punishing high achievers.Credit...Jim Wilson/The New York Times
Premised on the absurd notion that naturally gifted asian and white students simply have better opportunities than black and brown students - as opposed to differences in study habits, parental involvement, and cultural values - a draft plan to overhaul how math is taught across the state has set off a fierce debate, according to the NY Times.
Source
The draft proposal rejects the notion that some students are naturally gifted, and recommends against shifting certain students into gifted programs in middle school. It also proposes that math should not be 'colorblind' - and that teachers should use math lessons to explore social justice, "for example, by looking out for gender stereotypes in word problems, or applying math concepts to topics like immigration or inequality."
What?
Enter the backlash...
Critics - including hundreds of Californians working in STEM fields who signed an open letter opposing the plan - say it would punish high achieving students by limiting options gifted programs. According to the letter, the draft constitutes "an endless river of new pedagogical fads that effectively distort and displace actual math."
Even in heavily Democratic California — a state with six million public school students and an outsize influence on textbook publishing nationwide — the draft guidelines encountered scathing criticism, with charges that the framework would inject “woke” politics into a subject that is supposed to be practical and precise.
The battle over math pedagogy is a tale as old as multiplication tables.
"Math is math. Two plus two equals four," said Williamson M. Evers, a senior fellow at the Independent Institute and a former official with the Education Department during the administration of George W. Bush.An idea called “new math,” pitched as a more conceptual approach to the subject, had its heyday in the 1960s. About a decade ago, amid debates over the national Common Core standards, many parents bemoaned math exercises that they said seemed to dump line-by-line computation in favor of veritable hieroglyphs. -NYT
Will the adults in the room prevail?
[COMMENT: Equity is at the other end of the spectrum from competition. It may be more appropriate to teach toward equity in the lower grades where children are trying to grasp rudimentary basics, but even by third grade there can be significant differences among students in what they understand and know and how quickly they grasp new concepts.
Competition is a fact of life in the real world. Teaching to the lowest common denominator is unfair to the advanced student and is unhealthy to society at large. Life isn't fair, people are not equally endowed and that is a fact that also leads to beneficial societal outcomes. BTW, I suck at math.]
Maff is hard.ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
California's Attempt To Hobble Gifted Students Over 'Racial Disparities' Starting To Backfire
BY TYLER DURDEN
SATURDAY, NOV 06, 2021 - 10:30 PM
California's attempts to eliminate accelerated math courses for gifted students was a terrible idea from the beginning. Now it's beginning to backfire.
Critics of the draft said the authors were punishing high achievers.Credit...Jim Wilson/The New York Times
Premised on the absurd notion that naturally gifted asian and white students simply have better opportunities than black and brown students - as opposed to differences in study habits, parental involvement, and cultural values - a draft plan to overhaul how math is taught across the state has set off a fierce debate, according to the NY Times.
Source
The draft proposal rejects the notion that some students are naturally gifted, and recommends against shifting certain students into gifted programs in middle school. It also proposes that math should not be 'colorblind' - and that teachers should use math lessons to explore social justice, "for example, by looking out for gender stereotypes in word problems, or applying math concepts to topics like immigration or inequality."
What?
Enter the backlash...
Critics - including hundreds of Californians working in STEM fields who signed an open letter opposing the plan - say it would punish high achieving students by limiting options gifted programs. According to the letter, the draft constitutes "an endless river of new pedagogical fads that effectively distort and displace actual math."
"Math is math. Two plus two equals four," said Williamson M. Evers, a senior fellow at the Independent Institute and a former official with the Education Department during the administration of George W. Bush.
Will the adults in the room prevail?
[COMMENT: Equity is at the other end of the spectrum from competition. It may be more appropriate to teach toward equity in the lower grades where children are trying to grasp rudimentary basics, but even by third grade there can be significant differences among students in what they understand and know and how quickly they grasp new concepts.
Competition is a fact of life in the real world. Teaching to the lowest common denominator is unfair to the advanced student and is unhealthy to society at large. Life isn't fair, people are not equally endowed and that is a fact that also leads to beneficial societal outcomes. BTW, I suck at math.]
Sho nuff
marsh
On TB every waking moment

The Biden Regime Will Turn the Military on the People Unless We Push Back › American Greatness
“The coldest of all cold monsters.” That is what the modern state is. Nietzsche’s devastating analysis in Thus Spoke Zarathustra hit the nail on the head: the state is an engine of death.
 amgreatness.com
amgreatness.com
The Biden Regime Will Turn the Military on the People Unless We Push Back
What Christopher Rufo did with critical race theory must be done with the post-9/11 security state.
By Josiah Lippincott

November 6, 2021
“The coldest of all cold monsters.” That is what the modern state is. Nietzsche’s devastating analysis in Thus Spoke Zarathustra hit the nail on the head: the state is an engine of death. It wages war on the people, its agents are “annihilators” who seek the destruction of everything vital and potent.
All who witnessed the last 18 months of the COVID regime and the biomedical tyranny imposed by Joe Biden and his handlers implicitly understand what Nietzsche meant. The bureaucrats who make up the arm of the state, who serve this cold monster, hate the people. They make their lives miserable. Lockdowns, vax mandates, mask orders, critical race theory in schools, transgender bathrooms . . . the list goes on and on.
Ritual humiliation is the point. The agents of state power see themselves as the rightful masters of the people. To these creatures of the institutions, citizens are nothing but human resources to be bent to their malformed will.
This perverse view extends even to the American military. The time is coming, soon, in which the armed forces will be turned openly against the people. The Biden inauguration lockdown in D.C.—replete with checkpoints, thousands of national guardsmen, and the full weight of the nation’s security apparatus—was only a taste of things to come.
The Biden regime has no moral compunction against using force at home to impose its will. The barriers are practical, not ideological. Biden, in June of this year, mocked “gun-rights advocates” as a defense against tyranny. They would need “F-15s and nuclear weapons” to defeat the state, Biden claimed.
Implicit in this apparently weird statement is the acknowledgement that his administration would not hesitate to turn its full military might, including atomic bombs, against the populace in a war. The state, the coldest of cold monsters, headed by an endless mob of Anthony Faucis would not hesitate to impose its will in the most brutal manner possible.
The “pattern in the mount” is America’s wars overseas. The Bush Administration didn’t launch the war in Iraq and Afghanistan simply as punitive measures for 9/11. Rather, the aim was to radically transform the political and cultural way of life of these peoples. The American state declared war not on a few individuals or specific governments, but on entire modes of being. Afghanistan and Iraq would become democracies, even if they had to be bombed to smithereens to make that happen.
This hubristic project failed, of course. But not until after an enormous outpouring of money and blood. The United States used massive surveillance programs, biomedical data collection, secret prisons, extraordinary rendition, and a drumbeat of drone strikes to impose its will.
Everything our scientifically trained and sanctimonious elites did abroad to foreigners and “terrorists” will be done here at home. These chickens were always meant to come home to roost. The response of the bureaucracy, of the state, to 9/11 was to implement invasive security in every airport in America, spy on Americans without warrants, and launch bloody wars based on lies, with no accountability to boot.
It does not take a wild imagination to see the endgame. Tactics used against terrorists abroad will be used to beat down “insurrectionists” here at home. The decrepit conditions in D.C.’s “deplorables jail” and the ferocity with which federal law enforcement has gone after Boomers for wandering around the Capitol and making mischief shows the radicalization of our regime.
This has happened before. In the 1990s, the Clinton Administration had no qualms using armored vehicles, snipers, and heavy weapons against dissidents.
The FBI burned 76 men, women, and children alive at the Branch Davidian compound in Waco. At Ruby Ridge, a government sniper killed a mother in cold blood while she held her 10-month-old child.
As America becomes more divided and as the political class becomes more and more unhinged in its attempt to cling to power, the likelihood of state violence against the people increases. America is lucky. So far, there has been no real right-wing acts of terror against the regime. If there were, the situation might already have gotten out of hand.
The attempts by America’s national security apparatus to instigate provocations (in order to justify its own overreach) have failed . . . so far. The boobery surrounding the attempted “kidnapping plot” against Governor Gretchen Whitmer is instructive. The FBI managed to entrap a bunch of low-IQ rednecks in an elaborate plot to kidnap and possibly kill Whitmer, but it required immense effort and goading.
This could change in a heartbeat, however. The vaccine mandates, the endless drumbeat of anti-white racism from the Left, and the anti-Trump hysteria that animates the ruling class, is a toxic mixture. It could easily explode under the right circumstances.
In that situation, we can expect the Biden regime to deploy the military and national guard against its political enemies just as it did when it felt threatened by the January 6 “insurrection.” The Russiagate collusion hoax and General Mark Milley’s attempt to wrest control of the nation’s nuclear weapons from the elected president in the wake of the 2020 election show that our regime will no longer tolerate real opposition or dissent. We live in a regime of edicts and emergency “public health” measures. The Constitution is long dead.
If Americans on the Right are to prevent the use of the military and national security apparatus against the people, we must defang these institutions. The most powerful weapon at our disposal right now is mockery. We must strip America’s surveillance state and our bloated military industrial complex of honor and deference.
As a practical measure, we need to get public approval for the military to below 40 percent. Without a majority backing its actions, the armed forces cannot be used domestically without significant problems. What Christopher Rufo did with critical race theory must be done with the post-9/11 security state.
The Right needs to stay on message, pointing out over and over again that the military establishment is ideologically leftist and defends its own bureaucratic interest. The Pentagon has lost interest in winning wars and preserving the rights of the people. It exists to increase its own budget and follow “the process.” The bureaucrats who populate the military-industrial complex swamp feel no loyalty to ordinary Americans. They are loyal only to their own “expert” interests.
Patriotic Americans have no choice but to wage unceasing spiritual warfare against our degenerate and corrupt ruling class within the foreign policy establishment. Social media provides an excellent avenue for doing so. Twitter, for one, is populated with a horde of high and mid-level military officers who are both extremely liberal and extraordinarily hostile to the citizenry. They must be exposed for what they are.
My own presence on Twitter is bent entirely to this end—I have a mandate from heaven to fight back against this “coldest of cold monsters” using every spiritual weapon at my disposal. This mission has so far proven a success. My following continues to grow as I “ratio” multi-star generals, war planners, and recruiters who spend more time worrying about their fingernails, LARPing as military geniuses (despite repeated failure), and flying the flags of foreign powers in uniform.
This spiritual battle is just getting started, but there is no time to waste.
Americans must join the fray. Unless we push back, the use of America’s institutions of “national defense” will be turned against the people. Spiritedness in defense of our rights is our best weapon.
marsh
On TB every waking moment

‘Disingenuous’: Bill Maher Slams Leftist Prof Sneering Parents ‘Spooked By Critical Race Theory’
On Friday, HBO’s Bill Maher fired back at leftist Vanderbilt University professor Michael Eric Dyson after Dyson claimed parents were “spooked by Critical Race Theory.” Maher retorted, “I find that a disingenuous argument because I don’t think that is what people are objecting to.” Dyson stated...
‘Disingenuous’: Bill Maher Slams Leftist Prof Sneering Parents ‘Spooked By Critical Race Theory’
By Hank Berrien
Nov 7, 2021 DailyWire.com

On Friday, HBO’s Bill Maher fired back at leftist Vanderbilt University professor Michael Eric Dyson after Dyson claimed parents were “spooked by Critical Race Theory.” Maher retorted, “I find that a disingenuous argument because I don’t think that is what people are objecting to.”
Dyson stated, “The point is parents who were spooked by Critical Race Theory, none of whom can define it, when you ask them what it is, they don’t know.”
“I find that a disingenuous argument because I don’t think that is what people are objecting to,” Maher responded. “They are not objecting to black history being taught. There are other things going on in the schools.”
“Like what?” Dyson sneered.
“Like separating children by race and describing them as either oppressed or oppressor. I mean, there are children coming home who feel traumatized by this. That‘s what parents are objecting to,” Maher answered.
In January 2017, after black comedian Steve Harvey and football great Jim Brown met with former President Donald Trump, activist Marc Lamont Hill said, “It was a bunch of mediocre Negroes being dragged in front of TV as a photo op for Donald Trump’s exploitative campaign against black people.” Asked about Hill’s comments by Martha MacCallum of Fox News, Dyson began by claiming that whites had not been taught to think about race properly, intoning that in his new book what he wanted to do was to “invite white Americans into a conversation about race to think about how it’s constructed, about how white innocence, about white fragility, about white vulnerability are all thrown in there together, and how sometimes white people get resentful, understandably, being asked to talk about a subject they have no skills to talk about because they’ve not been practiced in it.”
Dyson added that former President Barack Obama’s presence “provoked a kind of nastiness, a viciousness. For instance, you can have legitimate disagreements with Barack Obama and not be accused of racism, but there’s no denying that a lot of the sentiment against Obama was racially driven.”
McCallum asked, “Are you saying Harvey is not the person for that conversation with Donald Trump?”
Dyson replied:
The same month Dyson told CNN, “Many African-American people say look we were introduced to terror long before 9/11 —the vicious police forces of America that have victimized us, and the way in which white supremacy operated.”'I’m saying that if you’re talking about serious issues of weight, values and gravitas with black America . . . Steve Harvey is not the point man for discussing policy in black America. I’m saying that there are many people who are practicing that, who are dealing with that every day, who have strategic advantages because they’ve been thinking about this: Steve Harvey is the attempt by Donald Trump to avoid with some serious weight and theological and theoretical and sociological analysis about what’s going on in the community.
In May 2018, debating famed psychologist Jordan Peterson, Dyson snapped, “This is what I’m saying to you: Why the rage, brah? … You’re doing well but you’re a mean, mad, white man.”
marsh
On TB every waking moment

Biden Admin Amassing Millions Of Records On US Gun Owners Amid New Crackdown On Firearms - CDM - Human Reporters • Not Machines
The Biden administration in just the past year alone stockpiled the records of more than 54 million U.S. gun owners.
 creativedestructionmedia.com
creativedestructionmedia.com
Biden Admin Amassing Millions Of Records On US Gun Owners Amid New Crackdown On Firearms
by CD Media StaffNovember 7, 202106406

Image by Houston Gun Show
The Biden administration in just the past year alone stockpiled the records of more than 54 million U.S. gun owners and is poised to drastically alter gun regulations to ensure that information on Americans who own firearms ultimately ends up in the federal government’s hands, according to internal Alcohol, Tobacco, and Firearms (ATF) documents obtained by the Washington Free Beacon.
The ATF in fiscal year 2021 processed 54.7 million out-of-business records, according to an internal ATF document obtained by the Gun Owners of America, a firearms advocacy group, and provided exclusively to the Free Beacon. When a licensed gun store goes out of business, its private records detailing gun transactions become ATF property and are stored at a federal site in West Virginia. This practice allows the federal government to stockpile scores of gun records and has drawn outrage from gun advocacy groups that say the government is using this information to create a national database of gun owners—which has long been prohibited under U.S. law.
The ATF obtained 53.8 million paper records and another 887,000 electronic records, according to the internal document that outlines ATF actions in fiscal year 2021. Gun activists described this figure as worryingly high and said it contributes to fears that the Biden administration is trying to keep track of all Americans who own firearms, in violation of federal statutes. The procurement of these records by the ATF comes as the Biden administration moves to alter current laws to ensure that gun records are stored in perpetuity. Currently, gun shops can destroy their records after 20 years, thereby preventing the ATF from accessing the information in the future…
To read more visit Washington Free Beacon.
marsh
On TB every waking moment

Thanks to New Diversity Policy Managers at One of the World's Largest Investment Firms, State Street Global Advisors, Will Need Permission to Hire White Males | The Gateway Pundit | by Joe Hoft
One of the largest and most profitable firms in the world will now require that managers get permission to hire white males in the company. Whatever happened to basing a man or woman’s worth on their character and abilities rather than on the color of their skin or their sex?
Thanks to New Diversity Policy Managers at One of the World’s Largest Investment Firms, State Street Global Advisors, Will Need Permission to Hire White Males
By Joe Hoft
Published November 8, 2021 at 12:20pm

One of the largest and most profitable firms in the world will now require that managers get permission to hire white males in the company.
Whatever happened to basing a man or woman’s worth on their character and abilities rather than on the color of their skin or their sex?
Martin Luther King Jr in his “I have a dream” speech shared the following:
Instead of adhering to Martin Luther King Jr’s speech, Americans are being subjected to a new kind of racism, covered with the lie that being racist against white males will somehow help solve the problem of racism.I have a dream that one day on the red hills of Georgia, the sons of former slaves and the sons of former slave owners will be able to sit down together at the table of brotherhood. I have a dream that one day, even the state of Mississippi, a state sweltering with the heat of injustice, sweltering with the heat of oppression, will be transformed into an oasis of freedom and justice. I have a dream that my four little children will one day live in a nation where they will not be judged by the color of our skin, but by the content of that character. I have a dream today.
Racism doesn’t solve racism.
Over the weekend it’s being reported that one of the largest investment firms in the world will mandate that before white males are hired, their hire must be approved by some higher-ups.
Leaders at one of the largest investment firms in the world, State Street Global Advisors, will need to ask permission to hire White men as it rolls out a diversity hiring initiative.
“This is now front and central for State Street — it’s on every senior executive’s scorecard,” said Jess McNicholas, the bank’s head of inclusion, diversity and corporate citizenship in London, according to the Sunday Times.
“All of our leaders have to demonstrate at their annual appraisals what they have done to improve female representation and the number of colleagues from ethnic-minority backgrounds.”
The company aims to triple the number of Black, Asian and other minority staff in senior positions by 2023, the Sunday Times reported.
If executives don’t meet the target, they will face lowered bonuses.
Recruiters will now have to establish panels of four or five employees, including a woman and a person with a minority background, when hiring middle management staff.
This is simply outrageous.
The white male is now being singled out and yet we should be doing the opposite. We should be measuring men and women by their character and abilities and not their sex and skin color.
marsh
On TB every waking moment

Dr. Glenn Loury schools Leftist on Bill Maher… Great clip…
Both clips are excellent. Dr. Glenn Loury is a conservative who teaches at Brown University. Bonus clip…
citizenfreepress.com
Dr. Glenn Loury schools Leftist on Bill Maher… Great clip…
Posted by Kane on November 8, 2021 4:11 pm
View: https://twitter.com/i/status/1456852781642371075
2:17 min
Both clips are excellent. Dr. Glenn Loury is a conservative who teaches at Brown University.
View: https://twitter.com/i/status/1456022417650946054
1;28 min

marsh
On TB every waking moment

Dropping the mic on CRT…
Virginia Delegate Nick Freitas drops the mic. Critical Race Theory, which is not taught in schools, is taught in every school.
citizenfreepress.com
Dropping the mic on CRT…
Posted by Kane on November 8, 2021 3:12 pm
View: https://twitter.com/i/status/1456738723404697604
2:16 min
View: https://twitter.com/i/status/1456738764013936646
1:03 min
Virginia Delegate Nick Freitas drops the mic.
Critical Race Theory, which is not taught in schools, is taught in every school.

marsh
On TB every waking moment
https://kunstler.com/cluster****-nation/woke-gets-whacked-but-hold-the-victory-lap/
CLUSTER**** NATION – BLOGNovember 5, 2021
Woke Gets Whacked — But Hold the Victory Lap
It begins to look like the 2021 elections put a decisive end to the Woke-Jacobin-Progressive reign-of-terror, and its demonic efforts to cancel the authority of truth in human affairs — truth being derived from reality. For years, in an ever-escalating campaign of coercion, persecution, and punishment, the WJPs made their own reality-optional “truth” and foolishly expected the nation to roll over for it. On Tuesday, voters all over the land, in effect, whapped the Party of Chaos upside its head with thirty inches of No. 6 rebar and said “no more.” Days later, the Wokesters are still seeing stars and planets blink in their temporal lobes.
The Virginia governor’s contest illustrated plainly and clearly what was at issue, all crystalized in the Loudoun County School Board’s idiotic behavior this past year. First was the sex module of the mess: A fifteen-year-old boy pretending to be a girl in a dress raped an actual teenage girl in a “Girls’” bathroom. The Loudoun County School Board covered it up so as not to interfere with its innovative gender confusion pedagogy. The boy rapist was transferred to another school where he committed the same crime all over again. Very bad optics. And WJP candidate Terry McAuliffe told parents to stay out of it, stupidly driving a stake through his own heart in the process.
Second was the Woke race module, namely Critical Race Theory, the principle that American society is hopelessly and systemically racist and that white people need to be punished for it. The School Board and its political allies denied that this doctrine of Marxist identity politics was being worked into the curriculum.
They were lying, of course, and stupidly, because it was very easy to prove.
Now, I’m going to tell you succinctly what is behind Critical Race Theory, and it’s going to hurt: After sixty-odd years of civil rights policy and legislation, a sizable cohort of African-Americans are not making it in this society and white WJPs (aka “liberals”) are stricken with guilt and shame at the failure of their efforts to uplift this group and heal the world. So, they’ve teamed up with the nation’s race hustlers to construct a scaffold of excuses for why this is so. The actual reasons for why this is so are taboo, namely, liberal deconstruction of American family life, unwillingness to prescribe behavioral norms, and self-sabotaging cultural choices such as the failure to promote the teaching of language skills as a primary task of public education — because ghetto English is more stigmatizing and economically disabling than skin color or any other feature of self-presentation, unless you are a professional comedian. That’s the cold, hard reality and that is what needs to change — but it won’t change as long as race-hustling (making money off the excuses) is considered “okay.”
Too many Americans see through the WJP sex-and-race nonsense and are now voting to evict it from the public square and run it out of the halls of power, at least at the state and local level. For now, though, it remains entrenched at the national level, in Washington, where it receives huge support from the very well-paid permanent bureaucracy that administers bad social policy. The 2021 election results suggest that the Woke Democrats will be run out of Congress and the White House in 2022 — if the USA can make it there without cracking up, which remains painfully uncertain under the toils of Covid-19.
The pandemic, so-called, invokes a dark suspicion of official misbehavior at a higher and more sinister level than the mere political inanities of Wokery. The public health officialdom has lied to the nation at every turn in this melodrama, and to the extent that many rational citizens think that the authorities are out to kill them. For instance, you have Dr. Fauci of the NIAID continuing to deny that he played any part in promoting gain-of-function research on viruses here and in the Wuhan lab. His latest dodge was to change the official definition of gain-of-function to an alphabet-salad of obfuscatory bullshit before a Senate committee — for which Senator Rand Paul once again accused him of lying and beseeched him to resign.
The CDC and the FDA have unleashed a set of untested vaccines on the public that have been shown to produce alarmingly high rates of adverse reactions, both disabling and leading to death. The CDC’s VAERS system for reporting all that is so janky that doctors can barely use it and the CDC refuses to fix it; meanwhile doctors are being punished for even attempting to report adverse reactions. The whole of medical officialdom has militated aggressively against early treatments of Covid-19 with cheap and easily available drugs, even firing doctors who attempt to use the protocols.
The entire approval process of the various vaccines has been rife with fraud, gamed statistics, sabotaged trials, bait-and-switch scams, and unaccountable manufacturing screw-ups — all immersed in a stench of moneygrubbing. The drug companies have refused to fully reveal the contents of the vaccines. Now they are ramping up an urgent campaign to vaccinate children following rushed and falsified clinical trials, with the statistical certainty that many more kids will be injured or will die from the vax than they would from Covid-19 itself.
Citizens have a right to object to this, and to the illegal vaccine “mandate” invoked by the pugnaciously stupid “Joe Biden” regime. There is an awful creeping suspicion in the USA and in other countries that people who have received vaccinations are beginning to present fatal cardiovascular and neurological illness in large numbers, and that an attempt is underway to cover all this up. There is likewise a growing body of evidence that the vaccines and “boosters” incrementally disable the human immune system so that later in the winter of 2021-2022 millions of people will be at risk of dying from Covid variants and virtually any other disease that comes along, including cancers. How many of us are prepared for that?
marsh
On TB every waking moment

‘Intentionally Tearing Us Apart’: Tulsi Gabbard Says ‘More And More Democrats Are Pushing’ Racial Division In America
Former Democratic Hawaii Rep. Tulsi Gabbard said Monday that
‘Intentionally Tearing Us Apart’: Tulsi Gabbard Says ‘More And More Democrats Are Pushing’ Racial Division In America

Fox News/Screenshot
DAVID KRAYDENOTTAWA BUREAU CHIEF
November 08, 20219:58 PM ET
During an appearance on “Tucker Carlson Tonight” on Monday, Former Democratic Hawaii Rep. Tulsi Gabbard said that “more and more Democrats are pushing” the racialization of American politics and it is “tearing” the nation apart.
WATCH:
Video on website 3:18 min
“Unfortunately as we see too often, more and more Democrats are pushing this racialization,” Gabbard told host and Daily Caller co-founder, Tucker Carlson.
“They are pushing more fomenting of anger and hatred and divisiveness that really is destroying us. It’s causing more suffering and more harm to the American people and the fabric of our country and undermining these values that our country was founded on,” she continued.
The former Democratic presidential candidate said this division can be seen “in how everything in our the country is being racialized: that this is an intentional strategy to tear us apart based on the color of our skin because they think that there’s some political gain to be had from it and don’t care at all about the destruction that they leave in their wake.”
Gabbard argued that “voters need to reject” the strategy just as they “choose leaders who do put the American people and our country first, who share that objective from both political parties.” She also said Democrats and Republicans must share one absolute political objective: doing what’s best for the U.S.
The former congresswoman pointed to the recent gubernatorial election in Virginia as an example of Democrats dividing Americans, and argued that candidate Terry McAuliffe “represented that fomenting of divisiveness, this racialization, and Virginia voters rejected that.”
As the Virginia election results were broadcast on Nov. 2, some members of the left-wing media said the Republicans were winning because of “white supremacy,” despite the election of Winsome Sears, a black woman, who is now the lieutenant governor-elect in the state.
")
Virginia Republican candidate for lieutenant governor Winsome Sears takes the stage during an election night rally at the Westfields Marriott Washington Dulles on November 02, 2021 in Chantilly, Virginia. Virginians went to the polls Tuesday to vote in the gubernatorial race that pitted Republican gubernatorial candidate Glenn Youngkin against Democratic gubernatorial candidate, former Virginia Gov. Terry McAuliffe. (Photo by Chip Somodevilla/Getty Images)
“[White supremacists] are dangerous, they’re dangerous to our national security because stoking that kind of soft white nationalism eventually leads to the hardcore stuff,” Reid said.
Gabbard has also specifically criticized Democratic California Rep. Maxine Waters for using race to “divide” American voters. She has also said Biden’s immigration policy is failing and that he should reconsider reintroducing some of former President Donald Trump’s policies to end an “open border.”
marsh
On TB every waking moment

Exclusive: Goodwill Is Pushing Critical Race Theory Through Staff Training
Goodwill Industries is pressuring its stores to adopt critical race theory-style training as part of its Diversity, Equity, and Inclusion initiative.
 thefederalist.com
thefederalist.com

Exclusive: Goodwill Is Pushing Critical Race Theory Through Staff Training
Goodwill Industries is pressuring its stores to adopt critical race theory-style training as part of its Diversity, Equity, and Inclusion initiative.

By Shawn Fleetwood
NOVEMBER 8, 2021
Goodwill Industries is purportedly pressuring its stores to adopt critical race theory-style training as part of the organization’s Diversity, Equity, and Inclusion (DEI) initiative.
According to former Goodwill of Southwestern Pennsylvania (SWPA) Retail Operations Manager Timothy O’Malley, his region first began discussions on how the company was going to be “different” following the 2020 presidential election.
“They stated that it was gonna be different and we were gonna make it about our community and our places,” he said. “That just turned out not to be true.”
O’Malley, who was employed with Goodwill for more than ten years, says that Goodwill of SWPA began holding “implicit bias training” for store managers in early 2021, which included a required “three to four hour” session led by a “racial equity trainer” in February.
“They started pushing us to recruit employees to be part of it,” he said. Implicit bias training is a common component of critical race theory and has been proven to be scientifically inaccurate to the point that some of the researchers who developed implicit bias tests have now repudiated them as wildly inaccurate and unreliable.
O’Malley also says he attended a “safe space meeting meant for asking questions” that same month, in which he raised “concerns” about the company’s woke policies that stemmed from Goodwill International’s recently fostered DEI initiative.
“I think they just assumed that I’d be on board with this because I foster children of all races and sexualities,” he said. “But I started asking questions about equality of outcome and equality of opportunity and I could tell that they weren’t too thrilled with me about that.”
“You were supposed to be able to offer your ideas, and so I suggested Thomas Sowell as an author to have some diversity of thought, and they told me that that’s not really what the DEI committee is about,” he added.
From a Goodwill employee website.
Following the committee’s pivot to discussions about “DEI language” and plans on how to “achieve equity,” O’Malley says he began asking questions regarding disciplinary outcomes.
“I said, so what you’re basically telling me is a white person and a black person can do the same thing, but a black person might be able to stay and a white person would get fired,” he said, while also claiming that Regional Director of Goodwill SWPA and North Central West Virginia Jessica McConnell told him, “That’s the point.”
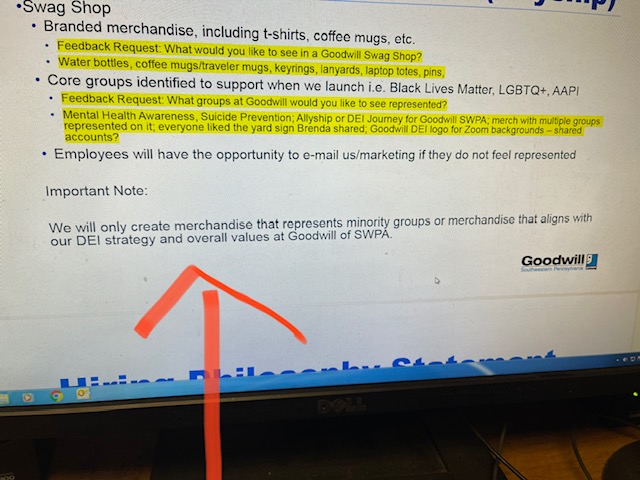
McConnell did not return The Federalist’s request for comment. The below screenshot shows Goodwill pledging to “only create merchandise” that represents members of preferred races.
Following months of numerous objections to the region’s leadership and an attempt to obtain a religious exemption from the company’s DEI push, O’Malley says he was terminated without cause in September 2021. O’Malley provided The Federalist a copy of his termination letter from Goodwill human resources.
“This was something I knew I wasn’t gonna win any friends by standing up for, but I just really feel that this is overreach by an employer trying to tell me how to feel,” he said. “I also really think it’s a betrayal of the donors’ trust.”
When pressed for details about his dismissal, Goodwill of SWPA’s vice president of marketing and development David Tobiczyk told The Federalist that the company “does not comment on specific personnel matters.”
The DEI Push Is Coming From The Top Down
The implementation of DEI appears not to be limited to Goodwill of SWPA. According to O’Malley, the company’s national arm, Goodwill Industries International (GII), has been “pushing the regions” to adopt DEI policies.
In June 2021, Goodwill International appointed Dr. Samantha-Rae Dickenson as its new director of diversity, equity, and inclusion, to “lead the development and promotion of DEI plans and implement workplace and initiatives and best practices” and “support the 156 local Goodwill nonprofit organizations in the U.S. and Canada by developing and curating DEI resources and strategies.”
“Goodwill’s entire mission and history has been to advance opportunities for people of all backgrounds in the workplace. Based on the rapidly changing nature of work, our commitment to DEI will entail ensuring that all people can benefit in the prosperity of our country by being equipped to compete for emerging opportunities in the workplace,” said GII CEO Steven C. Preston in a statement. “We are grateful to have Dr. Dickenson’s expertise as we continue our work to expand equitable opportunities for people in communities across our country.”
Dickenson’s so-called “expertise,” however, descends from her past embrace of ideologies such as critical race theory. Writing in a 2018 dissertation at the University of New England, Dickenson used “Critical Race Theory, Intersectionality Theory, and Black Feminist Theory as a theoretical framework to illustrate the occurrence of racial microaggressions that Black women face in the government sector.”
“According to the results of this study, societal standards can influence the behavior of Black women in a work setting and increase the occurrence of racial microaggressions which negatively affect their emotional views about themselves and their jobs, regardless of her level of education, age, socioeconomic status, type of job,” she wrote. “Results also illustrated that educating employees by holding all employees accountable for inappropriate actions and mentorship are effective methods that can help to reduce the occurrence of racial microaggressions in the workplace.”
In addition to hiring Dickenson and establishing a National DEI Task Force, Goodwill International has also taken steps to become more “intentional advocates for change” following the death of George Floyd. In May 2021, CEO Steven Preston confirmed that he signed the “CEO Action Pledge” in order to “provide a more supportive and inclusive workplace.”
According to the pledge, CEO’s commit to implementing and expanding “unconscious bias training,” which aims to help “employees recognize and minimize their blind spots” and to “facilitate more open and honest conversations.” CEO Action had previously hosted an event headlined by author of “White Fragility” Robin DiAngelo, who provided “insights on how to be #antiracist.”
Furthermore, Goodwill International has also released a three-part series on “microaggressions” that focuses on how employees can identify and address such actions in the workplace.
“Education is key to understanding how systemic discrimination and racism impacts each of us, pervades our daily lives, and negatively impacts the lives and futures of people of color,” the first post reads. “As we all learn ways to become anti-racist, it’s important to learn about microaggressions and how to address them in the workplace.”
“People who are on the receiving end of microaggressions or bias may be accused of being overly sensitive, not taking a joke or not accepting a statement intended as a compliment. Receiving a microaggression can be a stressful and negative emotional experience that contributes to a nonproductive and toxic working environment,” it added.
Goodwill Industries International did not return The Federalist’s multiple requests for comment about O’Malley’s allegations and the above screenshots.
marsh
On TB every waking moment

GOP Senatorial Candidate Blake Masters Nails It on The War Room - How to Save America from Big Tech (VIDEO) | The Gateway Pundit | by Jim Hoft
On Tuesday morning Arizona Senate candidate Blake Masters joined Steve Bannon on The War Room to discuss the existential threat of Big Tech on America’s future.
GOP Senatorial Candidate Blake Masters Nails It on The War Room – How to Save America from Big Tech (VIDEO)
By Jim Hoft
Published November 9, 2021 at 11:40am

On Tuesday morning Arizona Senate candidate Blake Masters joined Steve Bannon on The War Room to discuss the existential threat of Big Tech on America’s future.
Rumble video on website 2:59 min
Blake Masters, a 34-year-old chief operating officer at investment firm Thiel Capital and native Arizonan, launched his campaign for US Senator from Arizona in July. Since his launch, Blake has appeared on several media hits including The Gateway Pundit and The War Room.
For years Blake worked running Peter Thiel’s venture capital fund in Silicon Valley.
The fund today is worth upwards of $45 billion.
On Tuesday on The War Room Blake and Steve discussed the growing threat of the tech giant authoritarians.
Blake listed off five common-sense ideas on how to save America from these online tyrants.
1.) Take away the Section 230 immunity that is corporate welfare for Big Tech
2.) Make Facebook and Twitter common carriers – The phone company can’t kick you or me off for having a conservative conversation
3.) Google and Facebook should be broken up. No reason that they should have Facebook, What’s App, and Instagram so they can suck up your data
4.) We need comprehensive data privacy legislation – You own your data not giant international corporations
5.) Google can change elections via their search engine – is enemy number one when it comes to election integrity
These are excellent points that just make sense.
By the way— When you search BlakeMasters.com on Bing or DuckDuckGo the first search item that pops up is on car “brakes.”

And the BlakeMasters.com website is not even listed on the front page.
This is how the Tech Giants discriminate against conservatives.
(Google was actually better which was a surprise!)
Blake Masters went on to say we have 10-20 years to deal with the Tech Giants before we lose our country.
The Gateway Pundit believes we have less time than that.
This was an excellent segment on The War Room.
Rumble video on website 6:44 min
marsh
On TB every waking moment
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Virginia's Become 'Ground Zero' For Backlash Against Critical Race Theory Madness
TUESDAY, NOV 09, 2021 - 07:05 PM
Op-Ed authored by Eric Louw via The Epoch Times,
The election of a Republican governor in Virginia points to a winning formula in the upcoming mid-terms, a key component of which is empowering parents to fight back against Critical Race Theory’s (CRT) indoctrination of their children.
Gov-elect Glenn Youngkin’s victory was unexpected because the Democrats had won the governorship of Virginia for the last 12 years and the Democrat candidate, Terry McAuliffe, was popular.
More importantly, it looked like a major demographic shift had forever changed Virginian politics in favour of the Democrats, given the growth of a huge suburban population of Washington D.C. bureaucrats in northern Virginia.
For many Republicans, it felt like Virginia’s political game had forever been rigged against them by the arrival of these D.C. immigrants.

Republican gubernatorial candidate Glenn Youngkin (R-Va.) speaks during an Early Vote rally in Stafford, Va., Oct. 19, 2021. (Win McNamee/Getty Images)
But 2021 showed that even with this northern demographic challenge, Republicans can win Virginia if they can develop a powerful enough message.
Youngkin built such messages by exploiting the hubris, arrogance, and incompetence that has characterized the Democrats since Biden moved into the White House.
Essentially, he pledged to: support parents in their fight against CRT, fund the police, and cut red tape and tax.
So appealing were these pledges that they switched hundreds of thousands of votes from Democrat to Republican, especially independent voters.
Youngkin was also helped by Biden showing up to campaign alongside McAuliffe. This served to remind voters of the struggles of Biden’s administration, plus how it has empowered the woke-left’s CRT and police defunding agendas.
Additionally, Biden’s appearance also reminded voters that Biden does not look in charge.

President Joe Biden speaks during a press conference at the White House in Washington on Nov. 6, 2021. (Samuel Corum/Getty Images)
His $3 trillion “remake U.S. plan” is gridlocked in Washington. His migration policies caused chaos on the border. And anti-right-wing security on Washington’s streets only serves to make it look as if he does not even control his own capital.
But it would seem the core vote shifter was Youngkin’s standing up for parents’ rights to say no to the CRT bullies and to those teachers who want to indoctrinate students with it.
Youngkin correctly read the anti-CRT mood across his state.
After all, even in the blue northern suburbs of Loudoun County, some parents mobilized against their schools teaching CRT.
And so Youngkin has been rewarded with the governorship because he paid attention to the voices of Virginia parents, telling CRT-activists and woke-teachers: “I am not an oppressor, and I am not going to allow you to teach my children your toxic anti-white racism anymore.”
Essentially he produced a swing towards the Republicans in every part of Virginia by promising to ban CRT in Virginia schools.
Given the mounting parental backlash against the theory across America, it might be helpful to summarize the CRT worldview and objections to this radicalism.
CRT objects to how mainstream (white) Americans see themselves, their country and their history. CRT has the same objection to history as taught in Canada, Australia, and Europe.
Its solution is to teach a new kind of history.
Former Australian Prime Minister John Howard called this new history “the black armband view” in which everything before European colonialism was apparently wonderful, and everything since has been evil.
CRT argues Europeans invented race and racism to justify colonialism and slavery and effectively invented a new updated version of the old Marxist villain-victim idea. For Marxists, capitalists were villains, and workers were victims. For CRT, whites are villains, and blacks are victims.
Both models grow out of the resentments of the unsuccessful, but CRT’s answer is to tear down the successful and what they built.
The emergence of parental opposition to CRT in the schools reflects a growing realization that the theory represents a truly existential and revolutionary threat to the American way of life.
But CRT goes further than just wanting to deconstruct and reconstruct America and its way of life or take down statues. They demand all white individuals must recognize they are racists, which is built into them through language. They also demand that whites must apologize (and recompense black victims) for white racism, for white privilege, and for oppressing black people.
Within CRT logic, whites are apparently always inherently racist and inherently privileged. Blacks are always apparently oppressed and can never be racist.
If any white person points to the absurdity of these claims, this is taken a proof such a person is racist and “fragile.” CRT allows no escape from its closed circular argument.
Re-education appears to be the only solution, according to the theory.
Whites must be taught to recognize their individual “sickness” and the pathology of their society. Then taught to “be sorry,” to take the knee, and to be co-opted into CRT’s plan to deconstruct existing American society.
This re-education will take place in schools, universities and through compulsory staff training workshops.
Conveniently, CRT activists have created many jobs for themselves by running these workshops. Apparently, revolution can be profitable for some.
CRT is a revolutionary project designed to actively disrupt and break the language we use. It is enmeshed with another left-wing project called the “decolonization” of education and the “decolonization” of society.
These projects aim to undo the so-called evil of European colonialism plus deconstruct the work of the apparently evil white men who colonized and built America, Canada, and Australia.
Building CRT’s postcolonial world is a project as profoundly revolutionary as was Stalin’s communist project of building the “Soviet Man.”
Americans need to become aware of what such a project of re-writing their culture; their history, and their language will mean for them. If Americans want to see what “decolonization” of education and society means, just look at what the African National Congress has done in South Africa.
This is a project of erasure that is totalitarian in its vision.
What is remarkable is that left-leaning liberals cannot see how Orwellian this CRT re-education project is in the way it wants to replace “bad language” and “bad thinking” with new sanitized “social justice” words and “good thinking.”
Similarities can be found with Mao Ze Dong’s Cultural Revolution when communist witch hunts forced people to confess their “guilt.”
Youngkin’s victory in Virginia should give us all hope.
Let this be the beginning of an alliance of Republican politicians and parents who say they are tired of having their children come home from school brainwashed by CRT.
Let the message from Virginia be that enough is enough.
 Vandals attempt to pull down the statue of Andrew Jackson in Lafayette Square near the White House on June 22, 2020. (Tasos Katopodis/Getty Images)
Vandals attempt to pull down the statue of Andrew Jackson in Lafayette Square near the White House on June 22, 2020. (Tasos Katopodis/Getty Images)marsh
On TB every waking moment
Exclusive: Darrell Issa Reacts to YouTube Deleting Video that Called U.S. Vaccines Superior to Russia's
Rep. Darrel Issa told Breitbart News in an interview that he is the latest conservative voice silenced for spreading “medical misinformation.”
www.breitbart.com
Exclusive — Rep. Darrell Issa Speaks Out After Big Tech Ban: ‘We Have to Protect Free Speech’
 listens during a House Judiciary Subcommittee hearing on the proposed merger of CVS Health and Aetna, on Capitol Hill, February 27, 2018 in Washington, DC. CVS Health is planning a $69 billion deal to acquire Aetna, an American healthcare company. …")
JORDAN DIXON-HAMILTON9 Nov 20212
Rep. Darrell Issa told Breitbart News in an exclusive interview on Tuesday that he is the latest conservative voice silenced by big tech for spreading “medical misinformation.”

On Tuesday, Youtube removed a 20-minute speech Issa made addressing government employees and tech executives about open access to data. During his speech, he briefly highlighted the controversy surrounding the efficacy of Russia’s Sputnik vaccine for the coronavirus.
“What was amazing is it wasn’t what I said. It was who said it,” Issa said when asked what exactly in the speech got him censored.”
Issa compared both Russia’s and America’s vaccination efforts to the Cold War’s space race in his speech:
Issa noted that his point about the Russian vaccine program being inferior was reported by many mainstream outlets who criticized the Sputnik vaccine because it is not acceptable for international travel.But as I was talking about technology and our role and so on, I brought up the example of how Sputnik, in the case of the vaccine, arrived first, but not as good as America. Where we came into the space race and had to catch up, but we not only caught up, but we produce superior products. So in that analogy, which was very much a side note to the speech. I disparaged the Sputnik vaccine. Now that’s the only time I talked about health because this speech was not about vaccines or health or anything else. And they took it down and cited, specifically cited, these, you know, the health and vaccine, so I know why it was taken down.”

On Sunday, ABC News reported the problems with international travel because the Sputnik vaccine is not approved by the U.S. Food and Drug Administration:
“Oddly enough, I was in no way to disparage any other vaccines other than this relative one. So it wasn’t the subject of the speech. It was a side note, but it happened to be accurate, but it was a conservative talking about vaccine even tangentially and so they use [it] as an excuse [to] take out an entire 20 minute speech about open access to technology.”Sputnik itself said it was 60% effective until we came out with Pfizer in the 90s. And then they raised their effectiveness without any study, or third party. And so this is not controversial that Sputnik is an inferior product, and less well regarded even today, and yet they took it down over that statement.
Issa criticized Youtube’s medical misinformation policy because “They are using it to censor Republicans, conservatives, and their algorithm has no validity.” He also called out the hypocrisy of big tech for silencing his views even though the mainstream articles he got his information from remain online.
“Whether it’s Fauci or hundreds of other scientists or all of these major news organizations, none of them that I just noted was particularly right wing. They don’t get taken down for saying the same thing that, by the way, happens to be true,” Issa said.
“It doesn’t have to be true, to be protected by free speech. And so, you know, we we have to protect free speech, which we’re not doing until we stop the censoring of speech that we disagree with, that might be untrue,” Issa added.
Issa gave two real-world examples of what would happen if big tech became the arbiter of truth:
But I always give this example because I think it’s the easiest one. If Nancy Pelosi and Kevin McCarthy get up and talk about a bill, one of them could be taken down because it says the opposite of the other.
Issa emphasized that his comments did not call into question either the Pfizer, Moderna, or Johnson & Johnson vaccines, yet Youtube still took it down under the guise of “medical misinformation.”Okay. By definition, if you’re simply able to say we’re going to determine which one is the truth and take down the other one, then there is not any longer going to be free. speech as we know it. That means that when a prosecutor and a defense attorney, each talk about the defense attorneys client, one of them will have all their words taken off of YouTube and Google because obviously they’re going to decide which ones telling the truth. We can’t have this kind of censorship.”
“And in this case, I happen to be speaking in a way in which I was not disparaging American vaccines. I was not inaccurate, and yet I was taken down.
And in some ways, it’s the best example of taking someone down because of who they are not because of what they said.”
“We need to eliminate 230 as we know it,” Issa said when asked what needs to be done to protect the first amendment. “230” refers to section 230 of the Communications Decency Act, which grants internet platforms like Youtube broad immunity concerning third-party content. Section 230 was enacted in 1996 during the early years of internet browsing.
“I’m perfectly happy to have section 230 protect someone who leaves something up that I might find reprehensible that I might find false that I might find, in some way disparaging and I’m and I’m okay. With that. But I’m not okay with taking down something because a liberal writing an algorithm in San Jose decides that if your name is Darryl Issa or Jim Jordan, you need to disappear.”
Issa’s feelings are not partisan, as he said, “if it was Barney Frank or Nancy Pelosi, I would feel just as strongly that, you know, they’re wrong, but they have a right to be wrong.”
When asked if Congress intended for section 230 to allow platforms to censor U.S. politicians, Issa said, “they never intended to go as far as it’s gone. And for the most part, what they wanted it to do was to protect someone’s ability to say something that I might find reprehensible, that I might find objectionable, because ultimately, that’s the freedom that we want.”
Issa gave another example of how big tech’s censorship could lead to an infringement on the first amendment right to exercise religion freely:
Issa mentioned that he is not the only Republican legislator that’s been censored by big tech, with some even having their floor speeches get removed. “When one of our outspoken members you know, Congresswoman Taylor or something, gets taken down It’s like, ‘Well, this was this is a little edgy.’ And I believe that we need to stop that, she has every right to be edgy, he has every right to say what she believes.”I happen to be an Orthodox Christian, so I’m sort of an old faith. But you know, each of us believes in whatever religion you belong to beliefs by definition, that there is one truth and it’s the one that we practice. Can you can you imagine when they decide that there’s only one truth? And it’s probably atheism.
Issa noted that Google owns Youtube and the same censorship on the video streaming platform happens on the search engine. “And if you Google search ‘Sputnik vaccine’ you’re gonna find practically not a, zero article.” “But everything you read is going to say that this is not as good a vaccine if you can get an American vaccine get it is what all the articles say,” Issa said.
Issa concluded by saying, “that’s where we are, we’ve reached a point where even if they agree with you, they will take you down if they disagree with your politics.

marsh
On TB every waking moment

Biden Admin Moves to Scrap Trump Religious Liberty Rule
The Biden Department of Labor proposed rescinding a Trump-era rule that protects the religious liberty of faith-based organizations.
www.breitbart.com
Biden Admin Moves to Scrap Trump Rule Protecting Religious Liberty of Federal Contractors
355

DR. SUSAN BERRY9 Nov 2021382
The Biden Department of Labor (DOL) proposed rescinding a Trump administration rule that protects the religious liberty of faith-based organizations that contract with the federal government.
On Tuesday the DOL said it would roll back the Trump rule that went into effect on January 8 and allows religious groups that are federal contractors to specifically hire people who hold to their faith beliefs.
In August 2019, the Trump Labor Department announced the proposed rule intended to clarify that faith-based organizations “may make employment decisions consistent with their sincerely held religious tenets and beliefs without fear of sanction by the federal government.”
The Biden administration signaled it intended to overturn the rule, however, after civil rights organizations claimed it allowed discrimination against LGBTQ individuals in terms of hiring by faith-based groups.
The Biden administration is claiming the Trump rule “departed from” the Office of Federal Contract Compliance Programs’ (OFCCP) “longstanding policy and practice of applying principles and case law to interpret the exemption.”
Office of Federal Contract Compliance Programs Director Jenny R. Yang claimed:
But, Mary Beth Waddell, Family Research Council’s director of Federal Affairs for Family and Religious Liberty, said the Biden administration is actually “couching its change in terms of following precedent and the law to promote religious freedom,” and “doing the opposite.”The Office of Federal Contract Compliance Programs’ proposed rescission would protect against discrimination and safeguard principles of religious freedom. With this proposal, OFCCP would simply return to our policy and practice of considering the facts of each case and applying Title VII principles and case law and other applicable law.
Waddell said in a statement sent to Breitbart News:
“Religious freedom must protect the ability to practice and exercise sincerely held religious beliefs in the public square,” she added. Waddell noted the Trump administration:This Department of Labor proposed rule curtails the ability of religious individuals and entities to live out their faith in the public square. This is one of many choices the Biden administration has made to sideline religious freedom and elevate other policies in its place.
Waddell explained that, under the Trump-era rule, “religion” was defined as including “all aspects of religious observance and practice, as well as belief.” She went on:…understood this and did not tamper with what constituted a religious exemption in this rule, but rather defined the terms and added a rule of construction in favor of the broadest protection of religious exercise ‘permitted by the U.S. Constitution and law.’
The Biden administration’s move away from this definition is bad news.
American Atheists released a statement praising the Biden DOL’s proposed rule as it claimed the administration was “restoring workers’ freedom of religion.”Faith-based entities should not be denied government contracts and grants just because they want their employees to follow the same faith tenets they do. They should be allowed to freely exercise their religious freedom and run their business in accordance with the tenets of their faith.
“The government should never fund businesses that justify discrimination based on religious beliefs,” said Alison Gill, the group’s vice president for legal and policy. “And American taxpayers should never be forced to be complicit in discrimination.”
Nick Fish, president of American Atheists, added, “Finally, atheists, LGBTQ people, women, and religious minorities will see these important protections restored.”
“Let me be clear: The people who will be complaining about this change do not care about religious freedom—they only care about how they can use religion as a weapon against people different from them,” he stated.
But Terry Schilling, president of American Principles Project, said in a statement sent to Breitbart News that the proposed rescission of the Trump-era rule is a sign that “Joe Biden’s anti-American war on our fundamental freedoms continues.”
He elaborated:
“It’s obviously not going to work,” Schilling said. “Americans are sick and tired of the left’s radicalism, and there will be political hell to pay next November.”The administration is lying when they claim this move will prevent “discrimination.” In fact, it will do the very opposite: by eliminating critical religious liberty protections, the administration is declaring open season on persecuting religious organizations that dare to dissent from the left’s prevailing sexual orthodoxy. This is an affront to the First Amendment, but it shouldn’t surprise anyone — this is who they are. They oppose free speech. They reject the idea of religious freedom. The once great Democratic Party has been reduced to a bunch of would-be totalitarians hellbent on forcing everyone to submit to their insane mandates on gender, critical race theory, or even the latest politicized COVID “science.”
marsh
On TB every waking moment

Extremists pushing violence against Congress and health officials, DHS says
A new DHS anti-terror bulletin also noted how both foreign Islamic terrorists and domestic extremists want to exploit the U.S. exit from Afghanistan.
 www.nbcnews.com
www.nbcnews.com
Domestic extremists pushing violence against Congress, school and health officials, DHS bulletin says
A new DHS anti-terror bulletin also notes how both foreign Islamic terrorists and domestic extremists want to exploit the U.S. exit from Afghanistan.

A U.S. Capitol Police officer and K-9 perform an early morning security sweep in January 2020.J. Scott Applewhite / AP file
Nov. 10, 2021, 12:00 PM PST
By Ken Dilanian
WASHINGTON — Domestic extremists continue to exploit false narratives to promote violence online, calling for attacks on members of Congress, public health and school officials, even as they share information about how to build bombs, according to a new intelligence bulletin by the Department of Homeland Security that paints a picture of persistent danger.
The new National Terrorism Advisory System bulletin is expected to be released Wednesday afternoon, according to officials familiar with it. It replaces an existing bulletin published in August, which said that "ethnically motivated violent extremists and anti-government/anti-authority violent extremists will remain a national threat priority for the United States."
The new document includes a lot of the same language, according to a senior official who has read it. But it speaks to some new developments, including the exploitation of the American withdrawal from Afghanistan by both foreign terrorists and domestic racists.
Extremist groups focusing more on local issues post-January 6 .48 min

Foreign Islamic extremists "have sought to use events related to the U.S. withdrawal from Afghanistan to inspire potential followers to conduct attacks in the U.S.," the document says, and domestic extremists have sought to capitalize on concerns about the resettlement of Afghan refugees inside the U.S.
In general, the bulletin continues, "threats include those posed by individuals and small groups engaged in violence, including domestic violent extremists and those inspired or motivated by foreign terrorists and other malign foreign influences. These actors continue to exploit online forums to influence and spread violent extremist narratives and promote violent activity."
The ongoing pandemic continues to be a spark for violent rhetoric, DHS found, especially by those angered by mask and vaccine mandates and restrictions on normal activity.
If a new Covid variant emerges and new restrictions are imposed, "anti-government violent extremists could potentially use the new restrictions as a rationale to target government or public health facilities."
Man sentenced to 6 years in first sentence of kidnapping plot of Michigan Gov. Whitmer .24 min
Foreign intelligence services, foreign terrorist organizations and domestic violent extremists "continue to introduce, amplify and disseminate narratives online calling for violence," the bulletin says.
They also "continue to derive inspiration and obtain operational guidance regarding the use of IEDs and small arms through the consumption of information shared in online forums."
"Extremists have called for attacks on elected officials, political representatives, government facilities, law enforcement, religious communities, commercial facilities and perceived ideological opponents."
John Cohen, DHS's head of counterterrorism and intelligence, told a House committee last week that "the period of threat that we are in today is one of the most complex, volatile and dynamic that I have experienced in my career."
marsh
On TB every waking moment
New DHS Bulletin Warns 'Domestic Extremists' Are Pushing Violence Against Congress, School and Health Officials | The Gateway Pundit | by Cristina Laila
Here we go again.
New DHS Bulletin Warns ‘Domestic Extremists’ Are Pushing Violence Against Congress, School and Health Officials
By Cristina Laila
Published November 10, 2021 at 3:40pm
Here we go again.
The Department of Homeland Security is preparing to release a new ‘anti-terror’ bulletin warning that domestic extremists are pushing violence against Congress, school and health officials.
“Extremists have called for attacks on elected officials, political representatives, government facilities, law enforcement, religious communities, commercial facilities and perceived ideological opponents.” – the bulletin read according to NBC News.
The bulletin claims extremists may be angered if new Covid vaccine mandates are imposed: “anti-government violent extremists could potentially use the new restrictions as a rationale to target government or public health facilities.”
NBC News reported:
The new National Terrorism Advisory System bulletin is expected to be released Wednesday afternoon, according to officials familiar with it. It replaces an existing bulletin published in August, which said that “ethnically motivated violent extremists and anti-government/anti-authority violent extremists will remain a national threat priority for the United States.”
The new document includes a lot of the same language, according to a senior official who has read it. But it speaks to some new developments, including the exploitation of the American withdrawal from Afghanistan by both foreign terrorists and domestic racists.
In general, the bulletin continues, “threats include those posed by individuals and small groups engaged in violence, including domestic violent extremists and those inspired or motivated by foreign terrorists and other malign foreign influences. These actors continue to exploit online forums to influence and spread violent extremist narratives and promote violent activity.”
The ongoing pandemic continues to be a spark for violent rhetoric, DHS found, especially by those angered by mask and vaccine mandates and restrictions on normal activity.
In August, the DHS released a bulletin warning of an ‘increasing but modest’ threat of violence related to an online ‘conspiracy theory’ that Trump will be reinstated.Foreign intelligence services, foreign terrorist organizations and domestic violent extremists “continue to introduce, amplify and disseminate narratives online calling for violence,” the bulletin says.
The DHS also conceded there is no specific evidence of a credible plot.
marsh
On TB every waking moment

WaPo Op-Ed: 'Democrats Are Lying About Critical Race Theory'
The Washington Post published an opinion article on Tuesday titled "Democrats Are Lying About Critical Race Theory."
www.breitbart.com
Washington Post Op-Ed: ‘Democrats Are Lying About Critical Race Theory’
 being taught in schools at the Loudoun County Government center in Leesburg, Virginia on June 12, 2021. - Are you ready to take back our schools? Republican activist Patti Menders shouted at a rally opposing anti-racism teaching that …")
KATHERINE HAMILTON10 Nov 2021107
The Washington Post published an opinion article on Tuesday titled “Democrats Are Lying About Critical Race Theory,” an arguably unexpected headline from the far-left publication.
Writer Marc Thiessen criticized Democrats for “gaslighting American parents” about Critical Race Theory following Republican Glenn Youngkin’s win in the Virginia governor election. Thiessen writes a “twice-weekly column for The Post on foreign and domestic policy,” is a fellow at the American Enterprise Institute, and worked as a chief speechwriter for former President George W. Bush.
“It has become a refrain on the left and its media echo-chamber following Republican Glenn Youngkin’s victory in the Virginia governor’s race: Critical race theory is not being taught in schools,” Thiessen wrote, before noting several instances of corporate media falsely denying that the theory is being taught in schools. “…This is demonstrably false.”
Youngkin positioned himself as an enemy to the woke indoctrination of K-12 students, whereas Democrat Terry McAuliffe teamed up with far-leftists in the Democrat Party and even said parents should not tell schools what to teach their children.
Critical Race Theory being taught in schools was a top issue among Virginia voters, with 25 percent of 2,500 voters viewing the CRT debate as the single most important factor when deciding who to support for governor, a Fox News Voter Analysis survey found. During election and post-election coverage, corporate media personalities largely waffled between pretending CRT is not “real” and swinging in the opposite direction, conflating it with “America’s history” and advocating for its widespread teaching in schools.
Thiessan compiled a short list of leftist media lies following the election:
Thiessen then proceeded to link several examples of schools either teaching or training teachers to use the tenets of Critical Race Theory, several of which Breitbart News has extensively covered. He specifically detailed how Virginia’s Loudoun County Public Schools paid $314,000 for its teachers to be trained in Critical Race Theory by the Equity Collaborative. Thiessen wrote:PBS White House correspondent Yamiche Alcindor recently accused Republicans of winning by “lying about critical race theory.” Sen. Mark R. Warner (D-Va.) declared “there is not a school in Virginia that teaches critical race theory.” Those who say otherwise, we are told, are “dishonest,” hyping a “fake CRT threat,” promoting an “imaginary” issue to “manipulate low information people,” engaging in “race-baiting lies” and blowing a “racist dog whistle.”
He went on to report how the Virginia state superintendent of public instruction sent a memo to all school districts promoting Critical Race Theory training materials, and asserting:One Loudoun country parent filed the public record request to find out what took place in these sessions and obtained a set of talking points used by the Equity Collaborative to train Virginia teachers. They were encouraged not to “profess color blindness,” but rather to admit their own “racist, sexist, heterosexist, or other detrimental attitudes, beliefs, behaviors, and feelings” and acknowledge that “addressing one’s Whiteness (e.g., white privilege) is crucial for effective teaching.”
Thiessen concluded by calling the left’s CRT denial “intellectually dishonest,” and said “Democrats are gaslighting American parents” by telling them “not to believe what they can see with their own eyes.”CRT has proven an important analytic tool in the field of education, offering critical perspectives on race, and the causes, consequences and manifestations of race, racism, inequity, and the dynamics of power and privilege in schooling.
This is true in other states as well. In New York City, school administrators were required to undergo training sessions where they learned that “objectivity” and “individualism” were elements of “white-supremacy culture.” In California, students as young as six are being taught CRT-inspired lessons in white privilege and structural racism.
He wrote:
Thiessen argued that millions of parents were offered a closer look at what their children were learning when schools and moved instruction online during the pandemic, making Democrats’ attempts to deflect particularly ineffective.Just because grade-school students are not studying academic treatises on critical race theory does not mean it is not being taught in schools. Most of these students are also not reading Karl Marx, but if they were being instructed by teachers trained in Marxist thought to see everything through the prism of class struggle, they would be learning Marxism. Well, today children are being instructed by teachers trained in CRT to see everything through the prism of race; to believe that the United States is a systemically racist country; and to believe that society is divided into two classes — oppressors and oppressed — and that which you are is determined by the color of your skin. That is critical race theory.
“Many did not like what they saw. Nor did they like being told that the promotion of CRT is a figment of their imaginations, when in Virginia, it is right on the Department of Education’s website for all to see. So, they rose up to demand change,” he said.
Despite the overwhelming response from parents in various demographics, Thiessen said Democrats are “doubling down on the strategy of denigrating parents for raising legitimate concerns about their children’s education”
“Sorry, parents know that critical race theory is a real problem — and if Democrats continue telling parents their concerns are imaginary, they will continue to pay a price at the polls,” he concluded.
marsh
On TB every waking moment

CRT Co-Founder: Children Should Learn U.S. Is ‘Soaked in Blood of Theft’
Kimberlé Crenshaw, a CRT co-founder, said youth should “understand the ground upon which we stand is ground that’s soaked in blood of theft.”
www.breitbart.com
CRT Co-Founder: Children Should Learn U.S. Ground Is ‘Soaked in Blood of Theft’
")
JOSHUA KLEIN10 Nov 2021244
Professor Kimberlé Crenshaw, a co-founder of critical race theory (CRT), explained the importance of “looking at history to understand our present” while calling for youth to “understand the ground upon which we stand is ground that’s soaked in blood of theft.” She warned of the outcome if the “other side gets its way,” declaring “the road to authoritarianism will be paved through white supremacy.”
Crenshaw made her comments while appearing on British-American TV anchor Mehdi Hasan’s eponymous Sunday night MSNBC program, The Mehdi Hasan Show.
Hasan attributed Republican Glenn Youngkin’s recent “upset” victory in the Virginia governor race to the latter highlighting CRT — which the MSNBC host described as an “academic legal theory,” which is neither “critical” nor “theory” and which many “haters” admit they do not fully grasp.
“[Youngkin] went all in on CRT which is nothing if not a buzzword for all the racist words you are not allowed to say and for all the history you’re not allowed to teach about America’s past,” he said. “And surely the issue motivated parents.
But as a wedge issue, it really motivated white voters.”
“According to the exit polls: among voters who said, ‘parents should have a lot to say in what schools teach’ … Youngkin got 90 percent of the white vote and only 19 percent of the black vote,” Hasan added.
Crenshaw, who is also executive director for the African American Policy Forum and helped form CRT in the 1980s, described the concept as “a way of looking at the world that we have inherited after a legacy of segregation, of slavery, of Manifest Destiny, [and] of genocide.”
Calling it a link between “contemporary issues around racial inequality” and the “laws and policies that produce those very inequalities,” Crenshaw said, “it’s basically looking at the grounds upon which we stand, excavating those aspects of our history that have produced many of the problems that we still deal with.”
As an example, she cited current differences between black and white wealth being attributed to “how the suburbs were built and [how] they excluded African-Americans.”
“So it’s basically just looking at history to understand our present, that’s it,” she added, “but that’s not why they’re against it.”
Hasan then sought to clarify that CRT does not teach that white children are “oppressors,” made to “feel guilty” or “evil” for their white skin, and black children are “victims” — “as Republicans and even some self-proclaimed liberals like [HBO Real Time host] Bill Maher claim” it does.
In response, Crenshaw referred to such depictions as old and false arguments, though she avoids explaining how.

In this Feb. 2, 2019, file photo, Kimberle Crenshaw participates in the ‘Reconstruction: America After Civil War’ panel during the PBS presentation at the Television Critics Association Winter Press Tour at The Langham Huntington in Pasadena, Calif. Crenshaw, executive director of the African American Policy Forum, a social justice think tank based in New York City, was one of the early proponents of critical race theory. Initially, she says, it was “simply about telling a more complete story of who we are.” (Photo by Willy Sanjuan/Invision/AP, File)
“The oldest page in the book pushing back against racial integration has been to frame it as an attack on white people,” she said. “Civil rights laws were framed as discrimination against white people, integration of schools was framed as an attack on children, [and] reconstruction was framed as an attack on white women.”
“These arguments are the oldest ones in the book,” she added. “The only thing that is shocking about it, honestly, is that it is so easy to repeat them, it’s so easy to rehearse them.”
That is why, according to Crenshaw, Bill Maher “actually repeats that stuff — because he probably never learned what the truth is.”
Crenshaw also warned of the threat of authoritarianism in the event that “the story” is banned.
“If the other side gets its way, which is to completely ban conversations, books, [and] histories that tell the story, then a whole ‘nother generation will believe these lies and will not be able to understand that the true threat that we face right now is the threat of authoritarianism,” she said.
“That’s what this is about: the road to authoritarianism will be paved through white supremacy,” she added.
Calling responding to right-wing attacks on CRT education as a “catch 22,” she clarified that “no students in K-12 are being taught the Dred Scott case that said black people can never be Americans but what is taught is the history of slavery, a little bit of it; what is taught is the Trail of Tears, a little bit of it,” she said.
“So the point is that there are moments where our young people should learn our history. They should understand the ground upon which we stand is ground that’s soaked in blood of theft,” she added.
Claiming “racial appeals work in this country because there is still a lot of racism or at least racial resentment in America today,” Hasan followed up by saying that many, including Democrats, are “uncomfortable about suggesting a lot of white voters are susceptible to racist dog-whistles” and choose to hide behind euphemisms instead.
In response, Crenshaw claimed that was “precisely what critical race theory has been about all these years.”
“Many have been focused on how the inability to talk about race, the inability to see how it’s structured in our society, the inability to think about racism as anything other than moral turpitude or a psychological problem, has made it impossible for the media and others to identify racial projects when they’re happening,” she said.
“That is not an approach to deal with racism — we saw that on January 6 with the confederate flag marching right back into the capital,” she added. “So if we don’t have the ability to address racism, we won’t be able to save our democracy.”
Hasan concluded by claiming the “books they are always offended by or consider explicit … it always seems to be books from black authors or about black historical themes,” to which Crenshaw agreed, saying that books about social injustices “cause discomfort” and therefore are not welcome to be taught “so nobody has to find the actual definition of critical race theory to know what this is about.”
“This is what’s motivating the racial justice movements, so don’t let them take away what we want to pass on to the next generation: the ability to read our history and to know where the fight has to be,” she added.
The battle over CRT in schools has resulted in nationwide tension in recent months.
 being taught in schools at the Loudoun County Government center in Leesburg, Virginia on June 12, 2021. - Are you ready to take back our schools? Republican activist Patti Menders shouted at a rally opposing anti-racism teaching that critics like her say trains white children to see themselves as oppressors. Yes!, answered in unison the hundreds of demonstrators gathered this weekend near Washington to fight against critical race theory, the latest battleground of America's ongoing culture wars. The term critical race theory defines a strand of thought that appeared in American law schools in the late 1970s and which looks at racism as a system, enabled by laws and institutions, rather than at the level of individual prejudices. But critics use it as a catch-all phrase that attacks teachers' efforts to confront dark episodes in American history, including slavery and segregation, as well as to tackle racist stereotypes. (Photo by ANDREW CABALLERO-REYNOLDS / AFP) (Photo by ANDREW CABALLERO-REYNOLDS/AFP via Getty Images)")
People talk before the start of a rally against “critical race theory” (CRT) being taught in schools at the Loudoun County Government center in Leesburg, Virginia on June 12, 2021. (Photo by ANDREW CABALLERO-REYNOLDS/AFP via Getty Images)
The theory, which is promoted by many on the left, claims that American institutions — the government, economy, and culture — are based on racial hierarchy and aim at maintaining the dominance of white people, and even that which appears race-neutral is, on closer inspection, rooted in racism.
As a result, it urges reform in virtually all of the country’s institutions.
The theory’s architects have argued that the U.S. was founded on theft of land and labor, with federal law maintaining the unequal treatment of citizens by their race.
CRT advocates have also expressed the belief that race is culturally invented, not biological.
Last week, a Science, Technology, Engineering, Math (STEM) educator and administrator in the largest school district in Indiana addressed parents in a video in which he asserted when school officials say they are not teaching CRT, “we’re lying.”
In June, a former Democrat congressional candidate called on Americans to listen to black parents who oppose CRT “indoctrination” in schools, while calling on black Americans to reject the Democrat Party’s race narrative and, instead, realize “that their skin color is not a barrier to their progress,” adding that Democrats use race to galvanize black electorate support though many black Americans actually “have conservative ideals.”
marsh
On TB every waking moment

We're Going to Boycott Businesses That Are Anti-Conservative, Trump Tells Starnes - Todd Starnes
President Trump told radio host and best-selling author Todd Starnes that he is launching a program to boycott businesses that […]
 www.toddstarnes.com
www.toddstarnes.com
We’re Going to Boycott Businesses That Are Anti-Conservative, Trump Tells Starnes
Staff |
Nov 10, 2021
President Trump told radio host and best-selling author Todd Starnes that he is launching a program to boycott businesses that do not support conservative values. Starnes interviewed the president at his home in Mar-a-Lago. A partial transcript of Todd’s interview with the president is below.
TRUMP: We’re going to start something now very big program. We’re going to start boycotting businesses and recommending boycotts of businesses. There are more of us than there are of them. And I will tell you that when you have policies like no energy independence, no voter I.D., no borders, open borders attack the Second Amendment, so you don’t have any safety in your home. Sanctuary cities there’s no way there are 50-50 party. The only way they are 50-50 party is by misinformation and voter theft. Election integrity, lack of. There’s no way they’re a majority in terms of a real majority. And we’re going to start a big program on boycotting businesses that are against us, which should have been done a long time ago by Republicans. But they didn’t.
STARNES: I like that idea.
TRUMP: [01:03:47] Yeah.
STARNES: I do.
TRUMP: Well, it’s the only thing. I mean, they do it. I see these companies, some of these companies, like Coke and like Delta, they’re not radical left companies, but they’re threatened. They are threatened and the heads of the heads of them probably all voted for me. But they are threatened by these radical left lunatics and their companies are threatened. We’re not going to buy your product anymore. We’re going to say bad things about Coca-Cola. We’re going to say bad things about your airline and they say, man. And so they become woke. It’s a fake woke, but they become woke. So we’re going to we have more people than they do, and that’s the way it is.
marsh
On TB every waking moment

Goodwill Employee Terminated For Raising Concerns Over Anti-White CRT Staff Training Pushed By Walmart, AT&T, Delta, PulteGroup | The Gateway Pundit | by Alicia Powe
In addition to facing job loss for non-compliance with vaccine mandates, employees across the nation who dare oppose critical race theory risk being terminated as liberal business executives coerce their staff to undergo anti-white “equity and inclusion” training.
Goodwill Employee Terminated For Raising Concerns Over Anti-White CRT Staff Training Pushed By Walmart, AT&T, Delta, PulteGroup
By Alicia Powe
Published November 11, 2021 at 8:30am
In addition to facing job loss for non-compliance with vaccine mandates, employees across the nation who dare oppose critical race theory risk being terminated as liberal business executives coerce their staff to undergo anti-white “equity and inclusion” training.
Under the guise of “diversity” and “tolerance,” corporate CEOs are presenting their employees with an ultimatum: Go woke or go broke; comply with groupthink and denounce the US as a “white-supremacy system” or get canned.

Goodwill Industries is the latest corporation to make headlines over its institution of coercive critical race theory style classes.
Raising concerns about Goodwill’s bigoted “implicit bias training” resulted in former Goodwill of Southwestern Pennsylvania Retail Operations Manager Timothy O’Malley, getting fired.
Immediately after the 2020 election, Goodwill launched a Diversity, Equity, and Inclusion initiative. By February, all employees were instructed to attend a “three to four” hour training led by a “racial equity trainer,” O’Malley explained in an interview with the Federalist published on Monday.
“They started pushing us to recruit employees to be part of it,” he said. “I think they just assumed that I’d be on board with this because I foster children of all races and sexualities. But I started asking questions about equality of outcome and equality of opportunity and I could tell that they weren’t too thrilled with me about that.”

“You were supposed to be able to offer your ideas, and so I suggested Thomas Sowell as an author to have some diversity of thought, and they told me that that’s not really what the DEI committee is about,” he continued. “This was something I knew I wasn’t gonna win any friends by standing up for, but I just really feel that this is overreach by an employer trying to tell me how to feel. I also really think it’s a betrayal of the donors’ trust.”
O’Malley attended the company’s “safe space meeting” to push back against the company’s discriminatory “woke” policies.
“I said, so what you’re basically telling me is a white person and a black person can do the same thing, but a black person might be able to stay and a white person would get fired?” he asked.
“That’s the point,” Jessica McConnell, Regional Director of Goodwill SWPA and North Central West Virginia, retorted.
In a screenshot of a company-wide email, a Goodwill executive instructs the employees to “only create merchandise that represents minority groups or merchandise that aligns with our DEI agenda.”
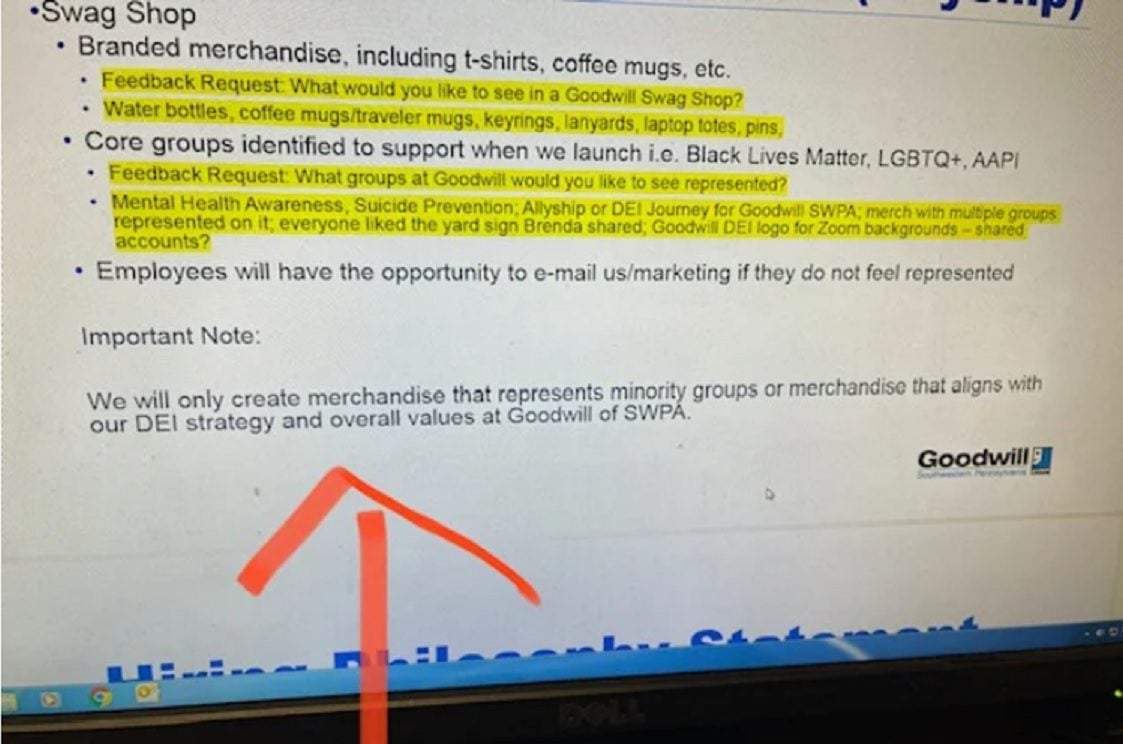
Refusal to comply with the racially divisive training led to O’Malley’s termination without cause in September.
The diversity training is being pushed from the top down by Goodwill Industries International CEO Steven C. Preston. In June, Preston appointed Dr. Samantha-Rae Dickenson as Goodwill’s national director of diversity, equity and inclusion to develop and implement “woke” workplace practices.
Dickenson authored a 2018 dissertation at the University of New England arguing employees must be held accountable for “racial microaggressions” against black women.
Preston is just one of a multitude of corporate CEOs who are forcing their employees to embrace and pay lip service to critical race theory.
A cache of leaked documents shows AT&T CEO John Stankey’s promotion of anti-white racism and critical race theory.
In the internal documents, published on Oct. 29 by City Journal’s Christopher Rufo, a senior fellow at the Manhattan Institute, Stankey directs his employees to attend “Listen. Understand. Act” training, a class that calls racism a “uniquely white trait.”

“White America, if you want to know who’s responsible for racism, look in the mirror,” reads the first page of AT&T’s Listen Understand Act internal portal.
The documents show employees of AT&T are also being asked to partake in a “21-Day Racial Equity Habit Challenge” that relies on the concepts of “whiteness,” “white privilege,” and “white supremacy.”
Rufo also obtained documents detailing Walmart’s critical race theory training.
During Walmarts CRT course, which implores staffers to stop thinking “white is right,” the corporate retail giant divides employees into racially segregated “affinity groups” because “people of color and white people have their own work to do in understanding and addressing racism.”
According to the training, racial minority employees suffer from “constructed racist oppression” and “internalized racial inferiority” which results in “self-hate,” “anger,” “rage” and “lowered self-esteem.”

Last week, Ryan Marshall, CEO of the PulteGroup, the nations’ third-largest home construction company lauded his companies new “Diversity Board” and the board’s development of “conscious bias training.”
A PulteGroup employee suspects Marshall is using the diversity struggle sessions as a way to weed out conservatives because minorities aren’t actually being promoted within the company amid the implementation of the new “inclusive” protocol.
“There doesn’t appear to be any accomplishments of the Diversity Board,” the insider told Big League Politics. The training is “likely just a smokescreen while black employees aren’t actually seen or heard from in any real way that changes this company.”
In March, Delta CEO Ed Bastian echoed talking points of the Democratic establishment regarding voter ID law. In a memo he issued to his employees, Bastian called a newly instated Georgia law requiring voters to present ID to voting is “unacceptable” and discriminatory against Black voters. In October, the CEO of the nation’s biggest airline announced that he is charging unvaccinated employees a $200-per-month surcharge in an effort to pressure more workers to get the shots.
Poll after poll shows that a majority of Americans reject woke corporations influencing everyday life, but when will we put our money where our mouth is?
marsh
On TB every waking moment
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Arizona School Board President Kept Secret Files On 'Wacko' Parents Opposed To Mandates And CRT
THURSDAY, NOV 11, 2021 - 04:40 PM
The president of the Scottsdale, Arizona Unified School District has come under fire for keeping a Google Drive full of private information on parents who oppose mask mandates and critical race theory.

The existence of the drive, which contained information on divorce filings, bankruptcies, phone numbers, and partial social security numbers, was discovered after a parent received an email from School Board President Jann-Michael Greenburg which included a screenshot of the URL, according to the Daily Caller.
Mother Kim Stafford uncovered a Google Drive link when school board President Jann-Michael Greenberg sent her an email accusing her of “anti-Semitic” comments against billionaire George Soros.
Greenburg sent Stafford a screenshot of his desktop, which included a since-deleted Google Drive URL reviewed by the Daily Caller. The drive was available to anyone who had the link.
Stafford shared the link with her friends, including mother Amanda Wray who told the Daily Caller she was “disgusted” when she saw that the drive included pictures of her 8 and 10-year-old daughters. -DC
 Screenshot/Google Drive (via the Daily Caller)
Screenshot/Google Drive (via the Daily Caller)The Google drive has been dubbed by some parents as an "online dossier."
Folders on the now-deleted drive included the names "SUSD Wackos," "Press Conference Psychos," and "Anti Mask Lunatics."
Contained within the "Press Conference Psychos" folder was a video of parents peacefully protesting Critical Race Theory - holding signs that read "CRT is Racist" and "SUSD We Demand Transparency."
The files took particular aim at "Community Advocacy Network" - a group of parents whose active Facebook pages were catalogued within Greenburg's 'dossier.' In addition to screenshots of their Facebook comments, the folder included photos of the parents with their spouses - and in some cases, their financial records."
 Screenshot/Google Drive
Screenshot/Google DriveOther posts detailed in the Google Drive include a PDF with members and moderators in CAN’s Facebook group, the personal documents that show portions of parents’ social security numbers, parents sharing pro-Trump signs or Thomas Sowell quotes, and one parent’s divorce proceeding.
The dossier also appeared to harbor opposition work against Amy Carney, a concerned parent who announced recently that she plans on running for Scottsdale Unified school board in Nov. 2022.
Carney told the Daily Caller that while Greenburg had access to the Google Drive, most of the information was procured and posted by Greenburg’s father, Mark Greenburg. The elder Greenburg is listed as the owner of the Google Drive, according to screenshots obtained by the Daily Caller.
The Greenburgs have been described by both Wray and Carney as "bullies" and "trolls" - adding that the elder Greenburg will go after parents who criticize the younger Greenburg.The elder Greenburg can be heard in bodycam footage reviewed by the Daily Caller calling Wray a “lunatic.” He also admitted that he pulled up to Wray’s car on his motorcycle with his license plate covered and said he had a private investigator “who’s writing down all of [the parents’ license] plates.” -DC
marsh
On TB every waking moment
The Critical Race Can Can…
Critical Race Theory, which isn’t taught in schools, is taught in every school in America Based teacher tells the …
citizenfreepress.com
The Critical Race Can Can…
Posted by Kane on November 11, 2021 7:21 pm
2:11 min
Critical Race Theory, which isn’t taught in schools, is taught in every school in America
or
View: https://twitter.com/i/status/1458890266102820907
2:12 min

marsh
On TB every waking moment

MSNBC's Wallace: Trump, Guns, Right-Wing Media Fueling Domestic Violence Threat Level
MSNBC anchor Nicolle Wallace said Thursday on her show "Deadline" that right-wing media, former President Donald Trump and guns were fueling the domestic extremism threat level. | Clips
www.breitbart.com
MSNBC’s Wallace: Trump, Guns, Right-Wing Media Fueling Domestic Violence Threat Level
PAM KEY11 Nov 2021186
Video on website 8:05 min
MSNBC anchor Nicolle Wallace said Thursday on her show “Deadline” that right-wing media, former President Donald Trump and guns were fueling the domestic extremism threat level.
Wallace said, “A domestic extremism threat unlike any other before in our country’s history looms over every facet of American life right now, today. It is fueled in-part by disgraced ex-president who is still lying about the fact that he lost the 2020 election fair and square. That disgraced ex-president now passes his days trying to stymy the bipartisan investigation into the worst attack on Congress in centuries, one that of course happened on his watch, and that he incited.”
She continued, “The committee’s investigation is playing out even as the domestic extremist threat to Congress and congress members remains. As the DHS notes in its latest terrorism bulletin made public yesterday. ‘Foreign and domestic threat actors have called for violence against elected officials, political representatives, government facilities, law enforcement, religious communities, or commercial facilities, and perceived ideological opponents.’ This threat is emboldened and empowered by a right-wing disinformation machine that includes members of Congress, people like Arizona Republican Paul Gosar, whose post depicting the murder of Democratic Congresswoman Alexandria Ocasio-Cortez was met with calls for censure and an ethics investigation from one party, the Democratic Party. But you guessed it, silence from Kevin McCarthy and his entire Republican leadership. It also includes right-wing media networks who glorify vigilantes, people like Kyle Rittenhouse, and supply a steady supply of toxic stew of grievance and violent rhetoric.”
After playing several Fox News and Newsmax clips, Wallace added, “Right-wing radicalization though is colliding with the proliferation of guns in America.”
Wallace concluded, “Folks, the lights are still flashing red. America’s gun crisis and the threat of domestic violent extremism is where we start this hour.”
marsh
On TB every waking moment

Memo Confirms National School Board Group ‘Actively Engaged’ with White House While Drafting ‘Domestic Terrorists’ Letter | National Review
The NSBA president said the organization also worked with DOJ and DHS before sending the letter.
Memo Confirms National School Board Group ‘Actively Engaged’ with White House While Drafting ‘Domestic Terrorists’ Letter
By CAROLINE DOWNEY
November 11, 2021 1:06 PM

Internal documents released Thursday confirm that the National School Boards Association coordinated with the White House before formally sending a letter to the Biden administration requesting federal intervention to probe and potentially prosecute parents for threatening school administrators.
In an October 12 memo, obtained by the nonprofit Parents Defending Education, NSBA president Viola Garcia stated that the organization had been “actively engaged” with federal departments including the White House, Department of Justice, Department of Homeland Security, before sending their letter to the president.
Chip Slaven, NSBA’s interim executive director, wrote in a September 29 email that the letter, which characterized parents as potential “domestic terrorists,” was revised to include details of “specific threats” at White House staff’s urging. As a result, the NSBA letter cited 24 local news outlet items detailing “threats” parents leveled against school board members, the vast majority of which did not constitute criminal threats.
In response to the letter, which the NSBA has since apologized for, Attorney General Merrick Garland issued a Department of Justice order mobilizing the FBI to coordinate with federal law enforcement to target parents deemed to be engaging in “threatening” behavior against school board members.
“In talks over the last several weeks with White House staff, they requested additional information on some of the specific threats, so the letter also details many of the incidents that have been occurring,” Slaven said in the email.
During a September 14 meeting, the executive directors of the group’s state chapters were notified that the NSBA had spoken with the White House about the letter that same day, Garcia claims in her memo. While the state chapters appear to have been given some advanced warning that a letter requesting federal intervention would be sent, they do not appear to have been given any specifics regarding the harsh language that would be used.
In addition to the state chapters being left in the dark, some members of the board of directors of the NSBA say they were not consulted or involved in the decision either, correspondence shows. Twenty-four NSBA state chapters distanced themselves from the letter amidst widespread condemnation from parents, and at least 12 state groups have formally disaffiliated from the parent organization.
Nicole Neily, president of Parents Defending Education, believes that Slaven and Garcia acted unilaterally and without the board’s consent in sending President Biden the letter.
“The NSBA board was not briefed. This was totally rogue,” she said.
In an October 11 email, Andrea Messina, executive director of the Florida state school board association, told Beverly Slough, a member of the NSBA board of directors, that she did not recall Slaven ever mentioning any communication with the White House during the September 14 meeting.
Referring to the headquarters’ plea for federal assistance to investigate parents, Messina said: “I do not recall his asking them for help at all and, like you, believe that even if I had missed it one of my colleagues would’ve picked up on it.”
In her reply, Slough affirmed that the board of directors were not clued in to the White House–NSBA collaboration. “As expected. I just cannot believe this part at all. Inconceivable that none of you would have referenced such a communication in all the back and forth,” she said.
In response to Garcia’s explanatory October memo, Pam Doyle, another member of the board of directors, pressed her on why the members of the board were left out of the loop.
“The members questioned why they were not consulted on the contents of the letter as well as the board’s involvement, or lack thereof. If I read the above paragraphs correctly, the origin of the letter began September 14th with a meeting with the White House staff, but fails to specify who met with the White House staff,” Doyle says.
Speaking on behalf of the board, Doyle also demanded to know which specific individual was behind the letter to the Biden administration and under what authority that individual sent it.
“It goes further to say ‘NSBA’ was preparing a letter to send to the President, failing once again to state the person that was preparing the letter, only an entity – NSBA.
The members asked specifically who wrote the letter, by what authority the letter was written, and who or how many states asked for federal intervention. This letter fails to adequately answer the specific questions about the lack of input from the members and Board in the letter to the President,” Doyle concludes.
marsh
On TB every waking moment
4:20 min
TUCKER & DHILLON: DOJ blew ‘fed. law, constitution, and civil rights’ ‘Deepest level of corruption’
Nov 11, 2021

Project Veritas
marsh
On TB every waking moment
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Medical Research Rapidly Adopts "Systemic Racism" As Truth, Risking Scientific Credibility, Part 1
FRIDAY, NOV 12, 2021 - 09:40 PM
By John Murawski of RealClearInvestigations, Part 1 of 2
Rejection used to be common for medical sociologist Thomas LaVeist when he tried to get his research published on the effects of racism on the health of black people. “Now,” said the 60-year-old dean of Tulane University’s School of Public Health & Tropical Medicine, “I have those same journals asking me to write articles for them.”
LaVeist’s experience illustrates the dramatic transformation in medical research, accelerating in the past few years. While few would dispute that black Americans are more prone to chronic health problems and have shorter life expectancies than whites, the medical community generally sought answers in biology, genetics and lifestyle. Research, like LaVeist’s, that focused on racism was frowned upon as lacking rigor or relevance, an amateurish detour from serious intellectual inquiry.
 Thomas LaVeist: His work focused on racism was once frowned upon as lacking rigor or relevance. Not any more.
Thomas LaVeist: His work focused on racism was once frowned upon as lacking rigor or relevance. Not any more.Today medical journal editors are clamoring for a racial lens and apologizing for what they call their past moral blindness. In recent years, and especially since Black Lives Matter protests erupted last year, systemic racism has been transformed from a fringe theory to a canonical truth.
Medical researchers are now able to offer a sweeping socio-political explanation for racial health disparities by citing the hundreds of peer-reviewed articles authored by LaVeist and a host of others, thus conferring upon the study of systemic racism the imprimatur of scholarly authority and even settled science.
This year, top officials at the National Institutes of Health issued an apology to all who have suffered from structural racism in biomedical research. The NIH, the nation’s largest funder of biomedical research, announced that it is dedicating $90 million to the study of health disparities and structural racism, engaging in more than 60 diversity and inclusion initiatives, and committing “every tool at our disposal to remediate the chronic problem of structural racism.”
In an August special issue dedicated to racial health disparities, the prestigious Journal of the American Medical Association stated that systemic racism is a scientific fact beyond dispute, and disagreeing on this point is “wrong,” “misguided” and “uninformed.” Systemic racism is a reality to be assumed in medical research rather than a sociological hypothesis to be tested by skeptical researchers.
Deemed incontestable, systemic racism provides the political rationale for “dismantling” — in the words of no less an authority than the National Institutes of Health — the social institutions and cultural standards that, according to the framework’s advocates, were constructed and are maintained to uphold white supremacy.
The consequences of ignoring this new prime directive for racially focused research were made abundantly clear this year when the top two editors of JAMA were pressured to resign after the organization ran a podcast that questioned whether systemic racism explains health disparities between blacks and other Americans.
“When JAMA sends a call for paper on structural racism, when the NIH director sends out an apology letter for racism in the NIH and when the CDC for the first time uses the term ‘racism,’ these are highest-level determinants of what research will be done in coming years in this country,” said Shervin Assari, an associate professor of family medicine and urban public health at Charles R. Drew University of Medicine and Science in Los Angeles, one of four historically black medical schools in the nation.
 Shervin Assari: Now the feds are "paying good money to the best researchers in this country who are competing to understand how structural racism works, rather than if it exists.”
Shervin Assari: Now the feds are "paying good money to the best researchers in this country who are competing to understand how structural racism works, rather than if it exists.”“This is the first time the NIH has issued a call for research on structural racism.
This is the first time JAMA fires an editor who said something wrong about racism,” said Assari, who has published more than 350 papers on race, social determinants and health equity. “Now NIH is paying good money to the best researchers in this country who are competing to understand how structural racism works, rather than if it exists.”
Systemic racism, generally unseen but known by its perceived effects, doesn’t directly cause diabetes, hypertension or depression, but it purportedly creates the living conditions in which chronic conditions opportunistically thrive, advocates say. Such living conditions include unsafe neighborhoods, aggressive policing, substandard schools, discriminatory workplaces, inferior medical care and the resulting stress, despair and self-destructive behavior, the theory states.
To institutionalize its new policy, JAMA is revising its peer review standards and diversifying its ranks to advance health care equity, a term that refers to narrowing or even eliminating racial health disparities in chronic conditions and life expectancies. Similar steps are being adopted throughout the medical profession — by the cluster-hiring of minority applicants, hiring of diversity and equity officers, and training staff on “white privilege,” implicit bias, microaggressions, and allyship.
A lead editorial in the August special issue, co-signed by 15 people, including JAMA’s newly installed executive editor and executive managing editor, along with other JAMA leaders, said all medical journals are morally obligated to assume systemic racism as a fact and document this fact in their research.
“At this point in the arc of medicine and scientific publication,” JAMA stated, “it is crucial for all journals to fulfill renewed editorial and journal missions that include a heightened and appropriate emphasis on equity and publication of information that addresses structural racism with the goal of overcoming its effects in medicine and health care.”
This rapid turn of events has blindsided traditional doctors, who are put off by the intense focus on race and the strong rhetoric.
“The spectacle of the gatekeepers of medical publications announcing a political blueprint that medical authors must follow — or else — is pretty breathtaking,” Thomas Huddle, who retired this year as professor at the medical school at the University of Alabama at Birmingham, said by email.

Thomas Huddle, dissenter: “The medical gatekeepers are in the grip of a moral panic.”
“The medical gatekeepers are in the grip of a moral panic,” said Huddle, who has published on medical ethics and edited several medical journals. “The JAMA convulsion over the podcast was positively Maoist in its fervor for achieving moral correctness and purging the impure.”
It's an open secret that some find the systemic explanation to be nothing more than leftist polemic, while others are skeptical it convincingly explains everything it claims to explain. These skeptics worry about the career implications of publicly dissenting from the new orthodoxy, but it's not inconceivable that blaming an entire national culture for racial disparities will prompt independent scholars and conservative think tanks to produce opposing research that explores black-on-black murder, racial disparities in IQ testing and other taboo subjects.
The dramatic transformation sweeping through the health care profession is not happening in a vacuum. It mirrors social justice movements committed to exposing structural racism that allegedly pervades education, criminal justice, the arts, hard sciences and other domains of U.S. society. Activists in those fields, as well as medicine, talk of dismantling white supremacy and other “structures” that operate by means of race-neutral laws and colorblind norms that cause racial and gender power imbalances and harm non-white groups.
Skeptical physicians say that medical journal editors are essentially replacing the scientific method with a political ideology, namely critical race theory, and leaving little room for alternative explanations — such as personal agency or cultural differences.
“There’s a tremendous amount of groupthink,” said Stanley Goldfarb, a former dean for curriculum who taught about kidney disease at the University of Pennsylvania medical school before retiring this summer. “If you don’t agree with all that, you’re a bad person.”
“This is an argument that you’re not allowed to have — that’s the problem here,” said Goldfarb, who has served on the editorial boards of three medical journals and was editor-in-chief of a nephrology journal.
Racial health disparities underlie the four-year gap in black-white life expectancy in the United States. The factors that contribute to this disparity include chronic conditions, unintentional injuries, suicide and homicide, which is the leading cause of death for black males aged 44 and younger. Scholars committed to the systemic racism explanation blame the disproportionately high crime rates in poor black neighborhoods on discrimination, substandard schools and other manifestations of systemic racism.
Part 1 of 2
marsh
On TB every waking moment
Part 2 of 2
The body of research into racial health disparities has broken into the mainstream after establishing credibility through the time-honored system of academic citations and referrals. Since LaVeist began his work in the 1990s, a small stream of articles has swelled into a critical mass that now allows medical researchers to assume systemic racism as a proven fact and cite the evidence in footnotes, as established knowledge, instead of arguing the case each time.
“When the weight of the evidence becomes so overwhelming that we reach consensus, we no longer continue to question whether or not [it is true],” LaVeist said. “We don’t question gravity anymore because the consensus is that gravity is a thing.”
One of the JAMA articles in the August special issue found that the major health care spending disparity is that whites spend more on dental, pharmaceutical, and outpatient care, while blacks spend more on emergency room and inpatient hospital care, suggesting that black people are more likely to be uninsured and otherwise lack access to routine medical care.
Instead of detailing the precise reasons that may explain this gap, the authors invoke previous articles: “There are many mechanisms that have already been identified that explain how structural racism shapes health and healthcare.”
In a phone interview, the lead author, Joseph Dieleman, associate professor of health metric sciences at the University of Washington in Seattle, said: “These are taken as a given by us. These are not to be debated, or being tested, in our analysis.”
Health Affairs, dubbed by a Washington Post columnist as “the bible of health policy,” is redoubling its focus on systemic racism, anti-racism, and equity, not only in its published content but also in attending to the racial makeup of its published authors and reviewers.
“We acknowledge that the dominant voices in our work are those with power and privilege,” Editor-in-Chief Alan Weil wrote in January. “Even as we have dramatically increased the volume of our content focused on equity, the narrative has primarily been written by those in power. We vow to change this.”
Weil, who was trained in critical legal theory, a precursor to critical race theory, as a Harvard law student in the 1980s, said in a phone interview that the concepts of merit and quality are often used to maintain power and privilege, and these structures must be examined for bias.
“We’re just talking about — forgive the language that is used by the believers — interrogating ourselves,” Weil said.
Systemic racism, a core tenet of critical race theory, doesn’t have a settled definition but it has broad applicability. One of the peculiar features of systemic racism is that the mechanism is not evident to those who are not initiated into the theory, but ubiquitous to its acolytes.
For best-selling and award-winning author Ibram X. Kendi, whose writings are considered essential reading at some medical schools, any disparity can signify racism. The concept can refer to all manner of disparate outcomes — in murder rates, arrest rates, life expectancies, education levels, school discipline, household income, standardized tests scores and grades — even in the fact that black people are nowhere to be seen in the corridor portraits of medical school dignitaries and are underrepresented in symphony orchestras.

Ibram X Kendi: Any disparity can signify racism.
“There is no ‘official’ definition of structural racism,” states a recent article in The New England Journal of Medicine. “All definitions make clear that racism is not simply the result of private prejudices held by individuals, but is also produced and reproduced by laws, rules, and practices, sanctioned and even implemented by various levels of government, and embedded in the economic system as well as in cultural and societal norms.”
One line of attack against the status quo is the movement to eliminate long-accepted practices to promote merit and excellence that, according to activists, operate as colorblind mechanisms to produce unequal outcomes: gifted and talented programs, gifted schools, and admissions tests for elite high schools, as well as standardized test scores for university admission. In medicine, the U.S. Medical Licensing Examination test is changing from a graded score to pass/fail to help minority students, while Northwestern University and its Feinberg School of Medicine are promoting diversity by eliminating a six-decade-old Honors Program in Medical Education.
Still, the concept provides special challenges for medicine. Unlike bacteria, for instance, systemic racism is an invisible force that can only be measured indirectly, by its perceived effects. Nevertheless, LaVeist is convinced that systemic racism is the best explanation for racial health disparities because the correlation of race and health is consistent across numerous studies for multiple chronic conditions.
“We cannot make direct causal inferences. The best we can do is look at plausible causality,” LaVeist said. “What we have is a case where once you’ve ruled out all of the plausible explanations, the only thing left is systemic racism.”
LaVeist and Weil agree that health and other disparities can have other causes than systemic racism, and good scholarship should be cognizant of other potential variables. LaVeist said that without allowing for other factors, people of color would have no free will, but it is important to note that African American culture is also shaped by white racism.
One of LaVeist’s early co-authored papers that was rejected by several journals before finding a publisher concluded that black people who experience rudeness at the hands of white people have longer life expectancies if they blame systemic racism, or some other external factor, for being treated disrespectfully.
An implication of the study: Even if the rude behavior by the white person isn’t caused by racism or an external factor, it’s strategically beneficial for black people to attribute the rudeness to someone else’s racism, boorishness or insensitivity, rather than blaming themselves.
“Yes — racism, or some other external attribution,” LaVeist said. “If you make an external attribution, that is going to be healthier than you thinking, ‘Oh they’re right, I am a bad person, I deserve to be mistreated.’”
Assari specializes in the study of “diminished returns” in quality of life and health that black people and other marginalized groups experience as they gain education and income in U.S. society. His research contends that black people reap fewer benefits — such as income and health — as they rise in education, compared to white people, which he attributes to structural racism. He has written half of the 300-some academic papers on that subject cited by the National Library of Medicine.
He makes connections that would not be self-evident to someone who lacks training in his specialty. One of his recent papers, published in the Journal of Health Economics, says that Americans are less likely to smoke as their income level rises. But that rule doesn’t hold for high-income Chinese Americans, who are more likely to smoke as they generate more income. So Assari postulates that upwardly mobile Chinese Americans resort to nicotine as a means of coping with the anti-Asian bias they encounter in this country’s elite institutions.
Yet, he also said that even though the anti-racist movement seems invincible now, overweening claims about systemic racism will eventually invite scholarly criticism, especially if equity policies and interventions now being implemented fail to deliver results.
“I think there will be a very strong backlash against critical race theory very soon,” Assari said. “I don’t think it is sustainable. And it is falsifiable. So there would be an anti-CRT movement among other group of social scientists.”
Nevertheless, Assari said systemic racism is a reliable theoretical framework because it parsimoniously explains the marginalization of many racial groups.
“This is one model which explains many of our observations,” Assari said.
“A theory is [reliable] when an observation or assumption holds regardless of the context, setting, place, population, design, sample. It is replicated many times across a diverse group of settings, age groups, resources, and outcomes.”
LaVeist said segregation, much of it rooted in historical practices such as redlining and Jim Crow, is the primary driver of disparities. Poor neighborhoods are generally more polluted, closer to highways and industrial zones, and have less access to quality restaurants, grocery stores, public schools, and green spaces. Such environments tend to breed despair, which leads to crime and an overly aggressive police response.
The constant stress of dealing with these hassles and micro-aggressions wears on the body, research into health disparities says, echoing arguments made by critical race theorists in the 1980s. One medical paper, published in The Lancet in 2017 and cited more than 1,500 times as of November, says that residential segregation is the foundation of structural racism, and notes that “growing research is linking interpersonal racism to various biomarkers of disease and well-being, including allostatic load, inflammatory markers, and hormonal dysregulation.”
There are those who say the medical establishment is not going far enough in this research direction.
The STAT News health information website reported in September that anti-racism and equity have become so trendy that “white scholars are colonizing research on health disparities.” According to the STAT investigation, white researchers are caught up in “a gold rush mentality” and “rushing to scoop up grants and publish papers.” The white scholars are replicating work done by black researchers without giving sufficient credit, a new form of exploitation practiced by “health equity tourists” and “opportunistic scientific carpetbaggers.”
One of the worst offenders: JAMA’s August special issue on health disparities. “Not one of the five research papers published in the issue included a Black lead or corresponding author, and just one lead author was Hispanic,” STAT reported.
Weil sympathizes with these concerns and said Health Affairs is creating a mentorship program to help scholars of color get their papers published in the journal. Weil, who said about 5% of submitted papers are accepted for publication at Health Affairs, is confident that dismantling power and privilege won’t necessitate compromising standards of excellence, and he considers such criticisms to be “generally false and intentionally inflammatory.”
“Equitable representation should be the outcome of an equitable process, not the jerry-rigged result of a change of standards for one group — that is not where we want to be,” Weil said. “So if the fix here is an equitable outcome by lowering standards for a certain group, our readers will notice, and that’s not the end point I’m looking for.”
Weil’s biggest concern is not that the anti-racist movement in medical research will go too far, but that the momentum and resolve will fizzle out.
“I think it’s very hard to tell where you are on a swinging pendulum when you’re in the middle of it,” he said. “I am much more concerned that this will become a rote exercise where everyone genuflects to anti-racism but does nothing about it, than I am that this is an overcorrection.”
The body of research into racial health disparities has broken into the mainstream after establishing credibility through the time-honored system of academic citations and referrals. Since LaVeist began his work in the 1990s, a small stream of articles has swelled into a critical mass that now allows medical researchers to assume systemic racism as a proven fact and cite the evidence in footnotes, as established knowledge, instead of arguing the case each time.
“When the weight of the evidence becomes so overwhelming that we reach consensus, we no longer continue to question whether or not [it is true],” LaVeist said. “We don’t question gravity anymore because the consensus is that gravity is a thing.”
One of the JAMA articles in the August special issue found that the major health care spending disparity is that whites spend more on dental, pharmaceutical, and outpatient care, while blacks spend more on emergency room and inpatient hospital care, suggesting that black people are more likely to be uninsured and otherwise lack access to routine medical care.
Instead of detailing the precise reasons that may explain this gap, the authors invoke previous articles: “There are many mechanisms that have already been identified that explain how structural racism shapes health and healthcare.”
In a phone interview, the lead author, Joseph Dieleman, associate professor of health metric sciences at the University of Washington in Seattle, said: “These are taken as a given by us. These are not to be debated, or being tested, in our analysis.”
Health Affairs, dubbed by a Washington Post columnist as “the bible of health policy,” is redoubling its focus on systemic racism, anti-racism, and equity, not only in its published content but also in attending to the racial makeup of its published authors and reviewers.
“We acknowledge that the dominant voices in our work are those with power and privilege,” Editor-in-Chief Alan Weil wrote in January. “Even as we have dramatically increased the volume of our content focused on equity, the narrative has primarily been written by those in power. We vow to change this.”
Weil, who was trained in critical legal theory, a precursor to critical race theory, as a Harvard law student in the 1980s, said in a phone interview that the concepts of merit and quality are often used to maintain power and privilege, and these structures must be examined for bias.
“We’re just talking about — forgive the language that is used by the believers — interrogating ourselves,” Weil said.
Systemic racism, a core tenet of critical race theory, doesn’t have a settled definition but it has broad applicability. One of the peculiar features of systemic racism is that the mechanism is not evident to those who are not initiated into the theory, but ubiquitous to its acolytes.
For best-selling and award-winning author Ibram X. Kendi, whose writings are considered essential reading at some medical schools, any disparity can signify racism. The concept can refer to all manner of disparate outcomes — in murder rates, arrest rates, life expectancies, education levels, school discipline, household income, standardized tests scores and grades — even in the fact that black people are nowhere to be seen in the corridor portraits of medical school dignitaries and are underrepresented in symphony orchestras.

Ibram X Kendi: Any disparity can signify racism.
“There is no ‘official’ definition of structural racism,” states a recent article in The New England Journal of Medicine. “All definitions make clear that racism is not simply the result of private prejudices held by individuals, but is also produced and reproduced by laws, rules, and practices, sanctioned and even implemented by various levels of government, and embedded in the economic system as well as in cultural and societal norms.”
One line of attack against the status quo is the movement to eliminate long-accepted practices to promote merit and excellence that, according to activists, operate as colorblind mechanisms to produce unequal outcomes: gifted and talented programs, gifted schools, and admissions tests for elite high schools, as well as standardized test scores for university admission. In medicine, the U.S. Medical Licensing Examination test is changing from a graded score to pass/fail to help minority students, while Northwestern University and its Feinberg School of Medicine are promoting diversity by eliminating a six-decade-old Honors Program in Medical Education.
Still, the concept provides special challenges for medicine. Unlike bacteria, for instance, systemic racism is an invisible force that can only be measured indirectly, by its perceived effects. Nevertheless, LaVeist is convinced that systemic racism is the best explanation for racial health disparities because the correlation of race and health is consistent across numerous studies for multiple chronic conditions.
“We cannot make direct causal inferences. The best we can do is look at plausible causality,” LaVeist said. “What we have is a case where once you’ve ruled out all of the plausible explanations, the only thing left is systemic racism.”
LaVeist and Weil agree that health and other disparities can have other causes than systemic racism, and good scholarship should be cognizant of other potential variables. LaVeist said that without allowing for other factors, people of color would have no free will, but it is important to note that African American culture is also shaped by white racism.
One of LaVeist’s early co-authored papers that was rejected by several journals before finding a publisher concluded that black people who experience rudeness at the hands of white people have longer life expectancies if they blame systemic racism, or some other external factor, for being treated disrespectfully.
An implication of the study: Even if the rude behavior by the white person isn’t caused by racism or an external factor, it’s strategically beneficial for black people to attribute the rudeness to someone else’s racism, boorishness or insensitivity, rather than blaming themselves.
“Yes — racism, or some other external attribution,” LaVeist said. “If you make an external attribution, that is going to be healthier than you thinking, ‘Oh they’re right, I am a bad person, I deserve to be mistreated.’”
Assari specializes in the study of “diminished returns” in quality of life and health that black people and other marginalized groups experience as they gain education and income in U.S. society. His research contends that black people reap fewer benefits — such as income and health — as they rise in education, compared to white people, which he attributes to structural racism. He has written half of the 300-some academic papers on that subject cited by the National Library of Medicine.
He makes connections that would not be self-evident to someone who lacks training in his specialty. One of his recent papers, published in the Journal of Health Economics, says that Americans are less likely to smoke as their income level rises. But that rule doesn’t hold for high-income Chinese Americans, who are more likely to smoke as they generate more income. So Assari postulates that upwardly mobile Chinese Americans resort to nicotine as a means of coping with the anti-Asian bias they encounter in this country’s elite institutions.
Yet, he also said that even though the anti-racist movement seems invincible now, overweening claims about systemic racism will eventually invite scholarly criticism, especially if equity policies and interventions now being implemented fail to deliver results.
“I think there will be a very strong backlash against critical race theory very soon,” Assari said. “I don’t think it is sustainable. And it is falsifiable. So there would be an anti-CRT movement among other group of social scientists.”
Nevertheless, Assari said systemic racism is a reliable theoretical framework because it parsimoniously explains the marginalization of many racial groups.
“This is one model which explains many of our observations,” Assari said.
“A theory is [reliable] when an observation or assumption holds regardless of the context, setting, place, population, design, sample. It is replicated many times across a diverse group of settings, age groups, resources, and outcomes.”
LaVeist said segregation, much of it rooted in historical practices such as redlining and Jim Crow, is the primary driver of disparities. Poor neighborhoods are generally more polluted, closer to highways and industrial zones, and have less access to quality restaurants, grocery stores, public schools, and green spaces. Such environments tend to breed despair, which leads to crime and an overly aggressive police response.
The constant stress of dealing with these hassles and micro-aggressions wears on the body, research into health disparities says, echoing arguments made by critical race theorists in the 1980s. One medical paper, published in The Lancet in 2017 and cited more than 1,500 times as of November, says that residential segregation is the foundation of structural racism, and notes that “growing research is linking interpersonal racism to various biomarkers of disease and well-being, including allostatic load, inflammatory markers, and hormonal dysregulation.”
There are those who say the medical establishment is not going far enough in this research direction.
The STAT News health information website reported in September that anti-racism and equity have become so trendy that “white scholars are colonizing research on health disparities.” According to the STAT investigation, white researchers are caught up in “a gold rush mentality” and “rushing to scoop up grants and publish papers.” The white scholars are replicating work done by black researchers without giving sufficient credit, a new form of exploitation practiced by “health equity tourists” and “opportunistic scientific carpetbaggers.”
One of the worst offenders: JAMA’s August special issue on health disparities. “Not one of the five research papers published in the issue included a Black lead or corresponding author, and just one lead author was Hispanic,” STAT reported.
Weil sympathizes with these concerns and said Health Affairs is creating a mentorship program to help scholars of color get their papers published in the journal. Weil, who said about 5% of submitted papers are accepted for publication at Health Affairs, is confident that dismantling power and privilege won’t necessitate compromising standards of excellence, and he considers such criticisms to be “generally false and intentionally inflammatory.”
“Equitable representation should be the outcome of an equitable process, not the jerry-rigged result of a change of standards for one group — that is not where we want to be,” Weil said. “So if the fix here is an equitable outcome by lowering standards for a certain group, our readers will notice, and that’s not the end point I’m looking for.”
Weil’s biggest concern is not that the anti-racist movement in medical research will go too far, but that the momentum and resolve will fizzle out.
“I think it’s very hard to tell where you are on a swinging pendulum when you’re in the middle of it,” he said. “I am much more concerned that this will become a rote exercise where everyone genuflects to anti-racism but does nothing about it, than I am that this is an overcorrection.”
marsh
On TB every waking moment

General Michael Flynn on Tucker Carlson: The Assaults on Our Freedoms Won't End Soon - Where are the Republican Leaders? (VIDEO) | The Gateway Pundit | by Jim Hoft
General Michael Flynn joined Tucker Carlson on Friday night following the news that former Chief Strategist for President Trump, Steve Bannon, was indicted by corrupt Attorney General Merrick Garland.
General Michael Flynn on Tucker Carlson: The Assaults on Our Freedoms Won’t End Soon – Where are the Republican Leaders? (VIDEO)
By Jim Hoft
Published November 12, 2021 at 8:10pm

General Michael Flynn joined Tucker Carlson on Friday night following the news that former Chief Strategist for President Trump, Steve Bannon, was indicted by corrupt Attorney General Merrick Garland.
Flynn, who was persecuted by the deep state, Democrat Party, and fake news mainstream media for years was asked to comment on the increasing threat of the radicals in charge of government and their cohorts in the media and Big Tech.
Flynn described the current crisis as a continual loss in our constitutional freedoms.
Ain’t that the truth. The Republican Party is completely worthless.General Michael Flynn: What I am not surprised at but I think Americans are surprised at, is the speed they are moving to do exactly what I said which is to take this country over. And we can’t kid ourselves, Tucker. That’s the direction that they are moving… The assault on our freedom of speech, our ability to peaceably protest the right to seek the truth in our elections, systems and processes. This is all at risk in our country today. And they don’t want us to be talking about these things… The other big question, the 60,000 foot view, is when does this stop or is ever going to stop? And I actually don’t see it stopping. I actually think we are going to continuously see this relentless pursuit on what I am going to call our rights from top to bottom. I actually advise everyone to go read the Bill of Rights because every single one of them is at risk under this particular regime that we are being dominated by… To me it’s this Republican establishment and these so-called Republican leaders. What I hear from the American people is they are looking for leadership out of the Republican Party and the Republican Party, they’re not doing it. They need to stand up and they’re just not doing it.
Via Tucker Carlson Tonight:
Rumble video 6:28 min
marsh
On TB every waking moment

The Public Education Complex Is Not On Our Side...It's Time For Good People To Get Ugly
By Kira Davis | Nov 12, 2021 3:30 PM ET

Renee Jones Schneider
I have been a school choice advocate and activist for nearly 20 years. I have long been of the opinion that the best way to push forward with school choice advocacy was to build bridges, educate people on the process, support legislation, stay away from heated rhetoric that turns away potential allies from other parts of the political spectrum, and never, ever, ever get unpleasant with your opponents.
Well, I’ve changed my mind.
It’s time to get unpleasant. Hell, it’s time to get downright ornery.
On Thursday The New York Post reported that the National School Board Association (NSBA) had actually had previous consultations with the White House before they sent their now infamous “domestic terrorists” memo.
A parent’s rights group, Parents Defending Education, unearthed an October memo from the NSBA that detailed at least one meeting at the White House just prior to the “domestic terrorists” letter they sent.
The memo, made public Thursday by the group Parents Defending Education, detailed at least one specific meeting with White House staff on Sept. 14, just over two weeks before the NSBA sent their letter to President Biden.
“In the September 14, 2021 meeting of the OSAED [Organization of State Association Executive Directors] liaison group, they were informed there had been a meeting with White House staff that morning and that NSBA was preparing to send a letter to the President,” the memo reads.
Merrick Garland’s public response was made on October 4th.“Subsequently, on September 17, 2021, the interim Executive Director emailed notice to the state association executive directors that indicated a letter requesting federal assistance would be sent.”
After reading the NYPost report, I was suddenly overcome with a sense of righteous indignation, moral outrage…just rage in general.
There’s no playing nice with these people. The whole thing has gotten out of hand and we parents are to blame. We got too comfortable. We believed the people we elected to our school boards were on our side. After all, they are our neighbors, they are our fellow citizens. These aren’t hardened politicians. They’re local concerned citizens who want to serve.
But we were wrong. They are not just regular citizens. They are not on our side. They are not here to serve.
You don’t run for school board because you (and I, we…we’re all culpable, here) have better things to do with your time. You don’t feel the need to meddle in public affairs. You’ve got church activities and your kids have sports and social events and you’re caring for aging parents and ailing neighbors. You’ve always left that work to the people who seem to really want to do it.
The problem is – as we’re finding out – that the people who are eager to do that work are the very people for whom power becomes irresistibly intoxicating.
They’re the same people who will call the snitch hotline to report a business that isn’t properly checking for masks or vaccine passports. They’re people who have traditionally had little power or control in their own lives, and so seek to wield it in some way over anyone they can. Those are the people who love public office, and they’ve ruined everything.
Everything was just fine for them as long as we were just showing up at the occasional school board meeting to argue about school lunches and half-days. They liked those interactions because that involved us asking for their help, asking for their permission.
Of course they hate that parents are suddenly getting loud and angry about the things they’ve allowed to happen to our schools and our students. It’s not the subject of the complaints that anger them, despite their protestations. It is that parents are suddenly realizing that school boards serve them, and not the other way around. The power dynamic is shifting and they hate it. Many school board members are nothing more than glorified meter maids and the more you protest that ticket, the more arrogant they get.
So, as much I advocate for grace and peaceful confrontation, I say the time has come to cause trouble, and keep causing it until we get what we want. Even in my beloved Bible there are stories of the people taking up the mantle of righteous anger and becoming rather unpleasant in service of beating back the enemy.
In this case, the enemy is tone-deaf school boards and their allies in the teachers unions.
These people are so unused to pushback that they think angry parents are terrorists…instead of dissatisfied customers. They are so cowardly that they can’t even stomach listening to someone critique the shitty jobs they’re doing. They are weak.
It’s time for us to be strong. It’s time for us to be disrupters. The squeaky wheels get the grease. We see that apply to progressive activists every single day. We’ve seen that apply to the brave and tireless parents in Loudoun County and other districts across the country.
The NSBA, the teachers unions, this administration – they are not on our side.
They just got comfortable with our complacency and were finally pushed too hard, too fast. We don’t think of simply holding our elected officials accountable as “war,” but if it’s war they see, then war is what they shall get.
It’s time for us to get in the mud, dig the trenches and start settling in for the long haul.
We are not the enemy. We are parents. We are the greatest advocates for our children and if we have to stand in front of our children to take the slings and arrows hurled at them from the power merchants, so be it.
The progressives in education have awakened a sleeping beast.
Hear us roar.
marsh
On TB every waking moment

WATCH: AZ Mother Targeted And Harassed By School Board: "We're TERRIFIED Of This Person Having Access To Our Information. My Eight And 10-Year-Old Daughters' Photos Were Found on Public Dossier" | The Gateway Pundit | by Jordan Conradson
A Scottsdale mother, Amanda Wray was recently targeted by local school board officials and Mark Greenburg, the father of School Board President Jann-Michael Greenburg.
WATCH: AZ Mother Targeted And Harassed By School Board: “We’re TERRIFIED Of This Person Having Access To Our Information. My Eight And 10-Year-Old Daughters’ Photos Were Found on Public Dossier”
By Jordan Conradson
Published November 13, 2021 at 7:15am
A Scottsdale mother, Amanda Wray was recently targeted by local school board officials and Mark Greenburg, the father of School Board President Jann-Michael Greenburg.
She was one of 50 parents whose private information including social security numbers, home documents, divorce documents, hidden camera footage, and other private personal information was harvested and publicized by Scottdale Unified School District officials.

The Gateway Pundit reported that Amanda was repeatedly harassed by Mark Greenburg, the crazed father of the school board president.
Greenburg also wished other victims of his stalking would die, saying “I’ll be so happy, I’ll have a f— party”.

"I Really Want Edmond to DIE. I’ll Be So Happy, I’ll Have a F*cking Party." - School Board Member's Deranged Father Stalks Parents And Wishes Them Dead | The Gateway Pundit | by Jordan Conradson
A Scottsdale School Board member was recently caught by parents harvesting their personal information and using his creepy father, Mark Greenburg to stalk them.
Amanda Wray was one of Greenburg’s top targets. She appeared on FOX and Friends yesterday to share her story.
FOX host: When you looked into this, what did you find?
Wray: Well, we found a digital dossier of more than 50 parents in our community, myself included with divorce decrees mortgage documents, background checks, social security numbers, it was really terrifying.
FOX host: I’m just curious, why would you be tracked?
Wray: Well, I became an advocate for increased transparency within our district and I became a vocal advocate for parental rights in education, and that made me a target. And our school board president has harassed and intimidated us. All parents in our district or you know hundreds of them and we’re terrified of this person having access to our information. My eight and 10-year-old daughters’ photos were found in Jan Miko Greenberg’s dossier.
FOX host: And the individual you just mentioned, is the President his father is also connected to this. They have emails that are attached to all of this; they deny any involvement. What can you tell us about these two guys?
Wray: Well, Jann-Michael revealed this Google Drive in an email to two parents. He sent an unsolicited email to those parents with the Google Drive address. He copied the Superintendent and the Board Vice President and to deny that it exists or deny connections, either somebody has access to his district email, or somebody is pretending to be him but I don’t know how he’s gonna explain how he’s not involved.
FOX host: What do you make of a statement like that? It seems like they are deflecting when they should be taken responsibility if all this is true.
Wray: Yeah, it’s weak. I understand he’s an elected official and the superintendent answers to him, but we need our superintendent and our other board members to step up, and hold this person accountable. If they really care about the district and our students and parents and trust, they need to call for his resignation. We don’t feel safe with him on the board.
FOX Host: Quickly. What’s your message to people who mess with kids like this, your kids, parents’ kids?
Wray: I tell you what. You know, parents are not the domestic terrorists here. We are the victims and I want all parents, grandparents, and community members to stand up and let these districts know that we’re not going to back down and be diminished.
These people are the real terrorists.We want to have rights, parental rights, and a voice within our school districts and be involved in our children’s education. And we’re not backing down.
Rumble video on website 3:49 min
marsh
On TB every waking moment

Washington Post Writer Jennifer Rubin Calls for "Rules" That Would Prohibit Media Outlets From Treating Republicans as "Normal" (VIDEO) | The Gateway Pundit | by Cristina Laila
Washington Post writer Jennifer Rubin on Saturday called for “rules” that would prohibit media outlets from treating Republicans as “normal.” Rubin attacked President Trump with lies and lashed out at Republican Reps Paul Gosar and Marjorie Taylor Greene.
Washington Post Writer Jennifer Rubin Calls for “Rules” That Would Prohibit Media Outlets From Treating Republicans as “Normal” (VIDEO)
By Cristina Laila
Published November 13, 2021 at 5:21pm

Washington Post writer Jennifer Rubin on Saturday called for “rules” that would prohibit media outlets from treating Republicans as “normal.”
Rubin attacked President Trump with lies and lashed out at Republican Reps Paul Gosar and Marjorie Taylor Greene.
Without providing any evidence whatsoever, Rubin claimed parents are threatening school board members with violence.
“You have to have new ground rules for the media. They have to stop treating Republicans like normal politicians. They are not normal politicians … This is a party that spends its entire time cooking up ridiculous culture memes and fanning violence and coming up with outright lies,” Rubin said Saturday on MSNBC.
VIDEO:
View: https://twitter.com/i/status/1459522826721972231
3:03 min