Alternatives to Allopathic medicine.
Case Report: Desmoid Tumor (Aggressive Fibromatosis), age 34, Male Fenbendazole Eradicates Non-Cancerous Tumor After Other Treatments Fail
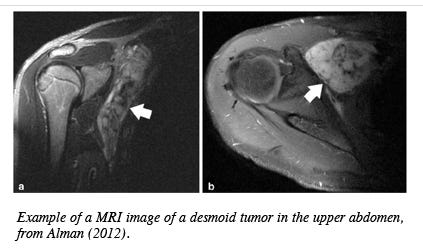
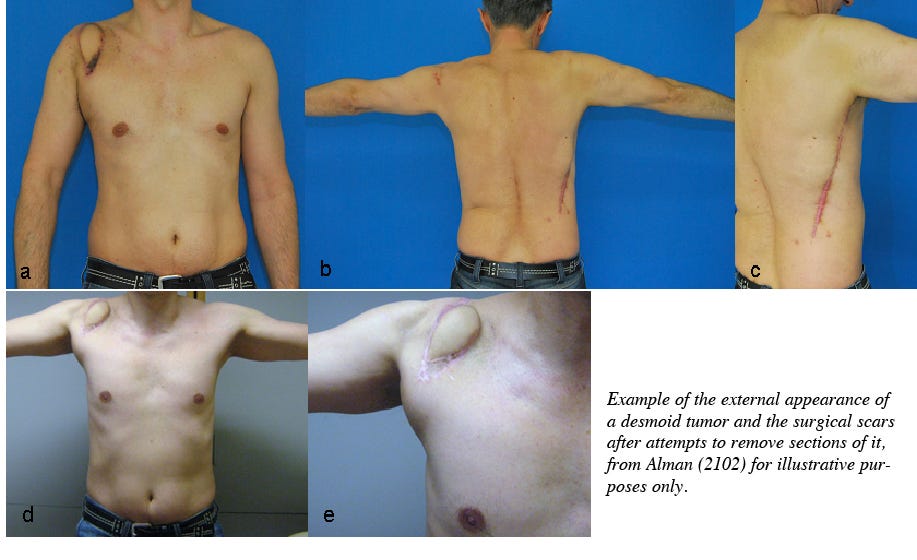
According to the Mayo Clinic, desmoid tumors are noncancerous growths that occur in the connective tissue. Desmoid tumors most often occur in the abdomen, arms and legs. Another term for desmoid tumors is aggressive fibromatosis. Please share this post with others who may be interested. Share Some desmoid tumors are slow growing and don't require immediate treatment. Others grow quickly and are treated with surgery, radiation therapy, chemotherapy or other drugs.
Case Report The following is a detailed Case Report of a man with an aggressive desmoid tumor and his experience in using fenbendazole to eradicate that tumor as told by his wife.
A. S., Winchester, VA July, 15, 2023 Q: It looks like that the timeframe was about a year until the tumor was gone (after starting fenbendazole), but that you suspect it may have been largely gone at 6 months...the first assessment after fenben was started? A: He is now 40 years old, the tumor was diagnosed when he was 34 years old, I guess that sort of paints a pretty good picture of the long and difficult journey this has been trying to overcome this. Up until a year after radiation/fenben treatment, they wouldn’t say “no evidence of disease”. There was some enhancement but we were told it was edema and likely scar tissue resulting from surgery/radiation. On his most recent scan, they actually did finally say “no evidence of disease”. I believe the fenbendazole worked within the first 6 months especially because his tumor was so diffuse and widespread, they were not able to access it, in its entirety, with neither surgery nor radiation. Leave a comment Q: Did the doctor(s) know your husband was taking fenben? Did they have any comments? A: He didn’t tell his oncologist until his most recent appointment in June. His doctor was intrigued and was just happy that he was finally tumor free. Q: One last question: did he take any supporting substances like vitamin E, CBD oil, etc. that some associate with the effectiveness of fenbendazole? A: He also took sweet wormwood, multivitamin, vitamin D3/K2, krill, bee propolis, magnesium. Summary Congratulations to this couple for thinking outside the box, taking control of a difficult situation, and making a potentially huge discovery in the process. Eradicating a tenacious tumor like this, that wraps itself around other structures making its complete removal almost impossible, is a remarkable feat. Why is this a potentially interesting discovery? In addition to identifying that fenbendazole is effective on desmoid tumors and potentially saving yet more heartache and lives, fenbendazole’s effectiveness on this “non-cancerous” growth is remarkable in other ways as well. It shines a spotlight on how we conceptualize what we consider cancerous growths, perhaps leading to a better understanding of how we can eradicate them. Is cancer conceptually much simpler than it appears? Have we overthought the complexity of cancer such that the obvious has been overlooked? Is cancer simply a “parasite” that shares similar structural vulnerabilities to other parasites, like the parasitic worm’s microtubule system affected by fenbendazole? Since it appears that non-cancerous desmoid tumors are similarly eradicated by fenbendazole, the category on which fenbendazole acts is broader than that of just “cancer” and/or “parasites”. Consider the following: • Invasive worms are not cancerous but their behavior is parasitic. They are eradicated by fenbendazole, an antiparasitic. • Desmoid tumor cells are not cancerous but their behavior is parasitic. These cells, too, are eradicated by fenbendazole. • Cancer cells should be considered parasitic because their behavior is such, and they are eradicated by fenbendazole. The host of diseases that we label collectively as cancer may be better characterized as parasitic infections. (Cancer viewed as a parasite is conceptually different to prior theories of cancer being caused by parasites, see Plimmer (1903), yes 1903!) It is not unreasonable to conclude that cancer is better characterized as a parasite based on its behavior as well as its selective susceptability to eradication by the antiparasitic medicine fenbendazole. Why does it matter how we conceptualize cancer? Because how we think about something determines the approach we will take towards dealing with it. Contemporary approaches to cancer research view the cells we call cancer as primarily a result of genetic malfunction or metabolic malfunction (Wishart, 2015). If we only look for genetic causes and therapies, and metabolic causes and therapies, guess what? We only find those causes and treatments! Think about it this way: if all one has in their toolbox is a hammer, everything tends to look like a nail. Which accounts for the less than perfect results from oncological research over the past 100+ years. Less than perfect because, while a hammer can be used for other tasks, it does them inefficiently, sloppily and perhaps detrimentally, causing more harm than good in the long run. More on this topic in future issues. Recharacterizing, or thinking about cancer as a potential parasite opens up the possibility of widespread acceptance of that fact that the antiparasitic medicine Fenbendazole Can Cure Cancer. Leave a comment Share Fenbendazole Can Cure Cancer References Alman, B. (2012). Desmoid Tumors: Are They Benign or Malignant?. In: Litchman, C. (eds) Desmoid Tumors. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-1685-8_13 Plimmer H. G. (1903). THE PARASITIC THEORY OF CANCER. British Medical Journal, 2(2241), 1511–1515. THE PARASITIC THEORY OF CANCER. Wishart, D. S. (2015). Is Cancer a Genetic Disease or a Metabolic Disease? eBioMedicine, 2, 478-479. https://doi.org/10.1016/j.ebiom.2015.05.022 |



")