In interviews with The Defender, pilots injured by COVID-19 vaccines said despite a “culture of fear and intimidation” they are compelled to speak out against vaccine mandates that rob pilots of their careers — and in some cases their lives.

childrenshealthdefense.org
05/06/22
•
COVID › NEWS
Exclusive: Pilots Injured by COVID Vaccines Speak Out: ‘I Will Probably Never Fly Again’
In interviews with The Defender, pilots injured by COVID-19 vaccines said despite a “culture of fear and intimidation” they are compelled to speak out against vaccine mandates that rob pilots of their careers — and in some cases their lives.
By
Michael Nevradakis, Ph.D.
As a commercial pilot, Bob Snow had long looked forward to seeing his daughter follow in his footsteps by helping her learn to fly an airplane.
However, having received the COVID-19 vaccine “under duress,” this dream is no longer a possibility for Snow.
“I will probably never fly again,” Snow said in a video he made about his story. “I was hoping to teach my daughter to fly. She wants to be a pilot. That will probably never happen, all courtesy of the vaccine.”
Snow is one of a growing number of pilots coming forward to share stories of injuries they experienced after getting a COVID-19 vaccine.
Some of these accounts are “hair-raising and deeply disturbing,” according to Maureen Steele, a paralegal and head of media relations for the John Pierce Law Firm.
The firm represents U.S. Freedom Flyers (USFF), an organization opposing vaccine and mask mandates for pilots and airline staff, in a series of legal actions against the U.S. Federal Aviation Administration (FAA) and several airlines.
Josh Yoder, a pilot with a major commercial airline, Army combat veteran and former flight medic, is a co-founder of USFF.
In a recent interview with The Defender, Yoder said the FAA has been aware of cases of pilots suffering vaccine injuries since at least December 2021, when the California-based Advocates for Citizens’ Rights hand-delivered an open letter to the FAA, major airlines and their insurers.
Yoder said USFF “has received hundreds of phone calls from airline employees who are experiencing adverse reactions post COVID-19 vaccination,” describing the stories as “heartbreaking.”
According to Yoder, the warnings contained in the letter, including testimony by “world-renowned experts,” were “completely ignored,” adding that “we are now beginning to see the consequences.”
This is leading an increasing number of pilots to “come forward to expose the truth regarding these toxic injections,” Yoder said.
The Defender recently reported on a series of reports that have been submitted to the Vaccine Adverse Event Reporting System, or VAERS, involving pilots who sustained severe injuries and side effects following the COVID-19 vaccine.
Congressional testimony from Cody Flint, an agricultural pilot who has logged more than 10,000 flight hours, was included in this letter.
“The FAA has created a powder keg and lit the fuse,” Flint said in an interview with The Defender.
“We are now seeing pilots experiencing blood clots, myocarditis, pericarditis, dizziness and confusion at rates never seen before. Pilots are losing their careers and having to call in sick or go on medical leave from medical issues developing almost immediately after vaccination.”
Vaccine-injured pilots share stories with The Defender
Several pilots, including Bob Snow, shared their stories with The Defender in a recent series of interviews.
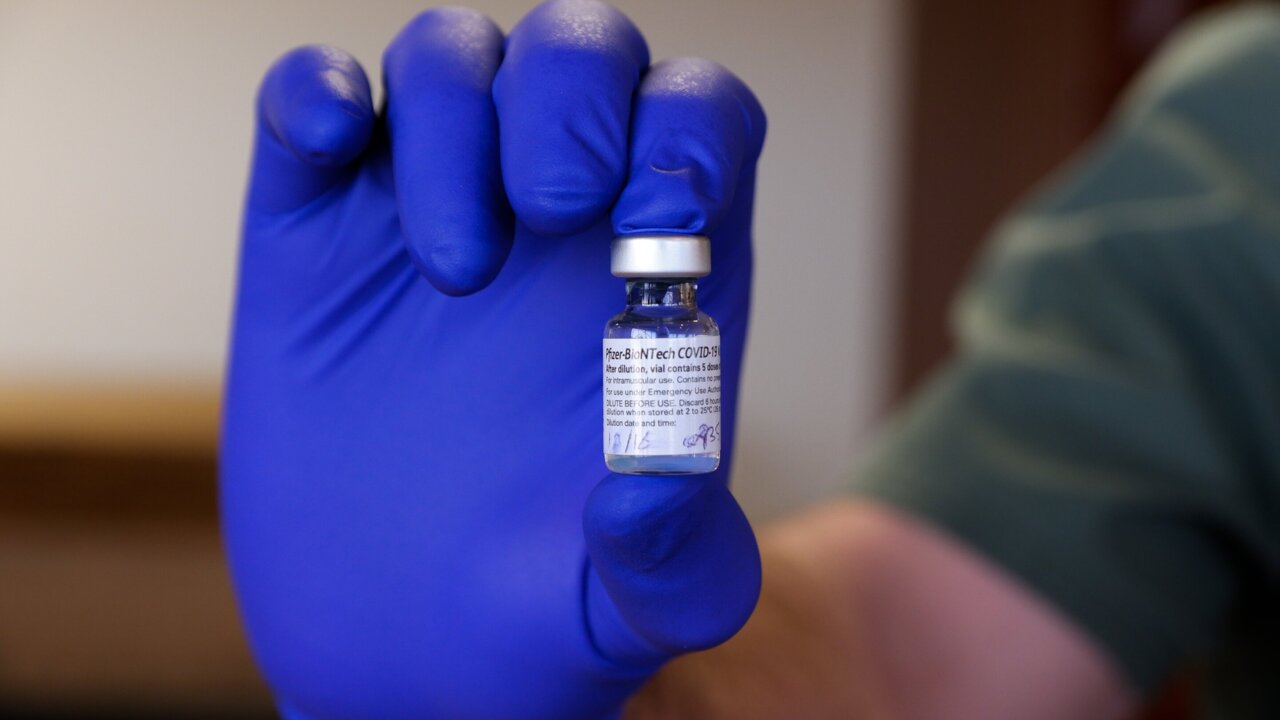
Snow, a captain with a major U.S. airline, told The Defender he received the Johnson & Johnson COVID-19 vaccine on Nov. 4, 2021, “as a result of an unambivalent company mandate to receive the vaccine or be terminated.”
According to Snow, he “began experiencing issues a little over two months” after receiving the vaccine. Due to a history of gastroenteritis, he underwent an endoscopy and an abdominal CT scan.
The results of the endoscopy were normal and Snow was awaiting the results of the CT scan when he suffered cardiac arrest on April 9, immediately after landing at Dallas-Forth Worth International Airport.
As Snow described it:
“I was very lucky to have collapsed when and where I did, as the aircraft was shut down at the gate post-flight and care was immediately provided.
“There was absolutely no warning preceding my collapse in the cockpit. It was literally as if someone ‘pulled the plug.’”
After receiving CPR and AED (automated external defibrillator) shocks to be revived, Snow spent almost a week in the hospital, where he was diagnosed with having sustained sudden cardiac arrest (SCA).
Medical studies indicate survival rates for out-of-hospital SCA cases are estimated at 10.8% to 11.4%.
Snow said:
“Needless to say, that’s not an encouraging number and I feel very, very lucky to have survived.
“Had this happened in a hotel, in flight, at home or almost anywhere else, I do not believe I would be here right now.”
Snow said prior to this incident, he had “no history of prior significant cardiac issues,” based on two EKGs (electrocardiograms) per year for each of the previous 10 years — none of which, according to Snow, “provided any indication of incipient issues that might lead to cardiac arrest.”
“I have no known family history to indicate a predisposition to developing significant cardiac issues at this point in my life,” Snow added.
Snow has been recuperating at home since April 15, while awaiting more tests that will provide a prognosis for his long-term survival.
However, it is likely that he will never fly again in any capacity.
Snow said, “[f]or now, it appears my flying career — indeed, likely all flying as a pilot — has come to a rapid and unexpected conclusion as SCA is a red flag to FAA medical certification.”
This, according to Snow, has resulted “in a significant loss of income and lifestyle,” adding that he has a college student and high school student at home and a non-working spouse who relied on his livelihood.
‘Last thing I remember is . . . praying I would make it’
Like Snow, Cody Flint had no prior medical history to indicate he was at risk.
“I have been extremely healthy my whole life with no underlying conditions,” said Flint, adding:
“As a pilot that held a second-class medical [certification], I was required to get a yearly FAA flight physical to show I was healthy enough to safely operate an airplane.
“I have renewed my medical every year since I was 17. The last FAA medical I received was on January 19, 2021. The medical showed I was perfectly healthy just 10 days before receiving the COVID-19 vaccine.”
Flint got his first (and only) dose of the Pfizer COVID-19 vaccine on Feb. 1, 2021. He told The Defender:
“Within 30 minutes, I developed a severe burning headache at the base of my skull and blurred vision. After a few hours, the pain was constant, but didn’t seem to be getting worse. I thought the pain would go away, eventually. It did not.”
Two days later began his seasonal job as an agricultural pilot, which typically runs from February to October of each year, Flint said.
He said:
“Approximately one hour into my flight, I felt my condition starting to rapidly decline and I was developing severe tunnel vision. I pulled my airplane up to turn around to head home and immediately felt an extreme burst of pressure in my skull and ears.”
Flint initially considered landing on a nearby highway, unsure he’d make it back to the airstrip, but chose not to so as not to put the public in danger.
Instead, according to Flint:
“The last thing I remember is seeing our airstrip from a few miles out and praying I would make it.
“Later, my coworkers told me I landed and immediately stopped my plane. They described me as being unresponsive, shaking and slumped over in my seat … I do not remember landing or being pulled from the plane.”
Flint said various doctors, including his longtime hometown doctor, refused to consider that his recent COVID-19 vaccination caused his symptoms. Instead, he was prescribed Meclizine for vertigo and Xanax for panic attacks.
According to Flint, doctors told him he would be “completely better within two days.” But two days later, Flint “could barely walk without falling over.”
Seeking a second opinion, Flint visited the Ear & Balance Institute in Louisiana, where he was diagnosed with left and right perilymphatic fistulas (a lesion in the inner ear), and highly elevated intracranial pressure due to swelling in his brainstem.
As Flint described it, “[m]y intracranial pressure had risen so high that it caused both of my inner ears to ‘blow out.’” Doctors told him this is usually caused by major head trauma.
“Obviously, I did not have head trauma,” said Flint. “What I did have, though, was an unapproved and experimental ‘vaccine’ just two days prior to suffering this bodily damage.”
“My doctors [at the Ear & Balance Institute] clearly stated my health issues were a direct result of a severe adverse reaction to the Pfizer COVID-19 vaccine,” he added.
Flint says he now cannot receive renewed medical certification from the FAA due to the injuries he sustained, the physical condition he is currently in and “the fact that I will be on the FAA-unapproved medicine Diamox for the foreseeable future.”
Like Snow, Flint believes “it is … highly unlikely that I’ll ever be able to fly again,” adding, “On most days, I am too dizzy to even safely drive a vehicle.”
Greg Pierson, like Snow and Flint, shared a similar story. A commercial pilot with a major U.S. airline that is also a federal contractor, he was mandated to get vaccinated.
Pierson told The Defender:
“I felt extremely pressured to consider getting vaccinated, even though I am adamant against any mandates that violate personal freedom choices.
“I did research and consulted several medical professionals regarding the associated risks.
“I have never had a flu shot in my lifetime, so this was not something I wanted to do. I reluctantly received the first dose of the Pfizer vaccine on August 26, 2021.”
For Pierson, the onset of symptoms was almost immediate, beginning “approximately 14 hours” after receiving the vaccine, when he experienced “an extremely erratic and highly elevated heart rate.”
Pierson visited a local emergency room, where he was diagnosed with atrial fibrillation. His condition was stabilized and he was soon discharged, though he remained on medication to help his heart return to a normal rhythm.
While Pierson says he has not experienced any further episodes, he nevertheless still has not been cleared to return to the cockpit.
“I successfully passed all the required protocols to re-obtain my certification that will allow me to return to work,” he said, adding the FAA has had his records and test results since Feb. 16, but he still hasn’t received a determination.
“I have been on disability since this occurrence, and combined with the leave, the personal and financial impacts have been significant,” Pierson said.
Pierson also described a similar experience to that of Flint, regarding the attitudes of some medical professionals regarding the possibility that his condition was brought on by the COVID-19 vaccine.
“When I brought the subject up to the ER cardiologist, that it was obvious what triggered my onset, she simply stated ‘s*it happens,’” Pierson said.
Widow describes husband’s last days
Snow, Flint and Pierson are fortunate in that they have managed to survive, even if their flying careers are in jeopardy.
But other pilots have not been so lucky.
American Airlines pilot Wilburn Wolfe suffered a major seizure following his COVID-19 vaccination, which cost him his life. Fortunately, Wolfe was not on duty when his seizure hit.
Claudia Wolfe, his widow, shared her late husband’s story with The Defender.
Wolfe, a former Marine just a few years from retirement, “was definitely against getting this vaccine but was put in the position to take it or lose his job as a captain,” Claudia Wolfe said.
He received the Johnson & Johnson vaccine on Nov. 9, 2021.
Claudia Wolfe told The Defender:
“[The] first 10 days were without any event … [on] day 11, it started with a migraine-like headache which got better that afternoon after taking a couple of aspirin.
“Unfortunately, the migraine came back and he was hoping that it’s nothing else but a migraine.
“On November 22, 13 days after the COVID vaccine, he had a seizure. When paramedics arrived and my husband came out of the seizure, he was paralyzed on his right side, arm and leg, and was taken to the emergency room.”
At the emergency room, a CT scan showed he was experiencing brain bleeding, and he was admitted into intensive care. There, according to Claudia Wolfe, “he continued to have convulsions on his right hand … shortly after he was admitted, he had another seizure and doctors decided to sedate him and put him on a ventilator.”
“That was the last time I talked to my husband, before the seizure in the ICU,” Claudia Wolfe said.
Wolfe never regained consciousness and died on Nov. 26, 2021 — only 17 days after receiving the COVID-19 vaccine. Even if he had survived, he likely would not have been able to work as a pilot again.
As Claudia Wolfe explained:
“Doctors told me that he couldn’t work as a pilot anymore because he would have to be on seizure medication.
“But as the bleeding continued to spread I was told that he probably would not recognize me or his family and he probably would need a 24-hour facility to help him.
“This man was so strong and never needed a doctor, he was never sick enough to need one, and [he] just had a physical a couple months prior for his job as a pilot.”
Pilots describe culture of fear and reluctance to come forward
Pilots who spoke to The Defender described a culture of intimidation that has led to many of their colleagues fearing professional or personal consequences if they speak publicly about injuries following COVID-19 vaccination.
According to Yoder, “Many pilots and other airline employees capitulated to the tactics of threats, harassment and intimidation perpetrated by the very companies they serve.”
Yoder described airlines, as well as aviation industry unions, as “state actors” illegally “working in lockstep with the U.S. government” to “enforce unconstitutional mandates via a culture of fear.”
Snow told The Defender several of his colleagues shared stories of vaccine injuries with him:
“Since my SCA I have heard from several other airline personnel regarding potential vaccine injuries up to and including cardiac issues (chest pain and myocarditis).
“Many crewmembers are very reluctant to divulge potential significant health issues for fear of losing their FAA medical certification and, potentially, their careers.”
According to Snow, such fear exists “due to both concern for one’s career and also the fear of being portrayed as a vaccine skeptic.”
“There seems to be genuine reluctance on the part of corporations, businesses, government and the medical community in general to acknowledge the potential for COVID vaccine injury,” Snow said.
Claudia Wolfe also shared her experience, stating that following her husband’s death, she learned “of others that died after the COVID vaccine,” adding that “not many talk about it or believe this vaccine can harm or kill you.”
Pierson also expressed concerns, telling The Defender, “Some things I have stated publicly could have consequences in this regard.”
This culture of intimidation appears to extend beyond just accusations of being a “vaccine skeptic.”
Steele described incidents of airline employees’ non-work and online activities seemingly being monitored by their employers, who are then using this as a justification to question or harass those employees.
“I believe the airlines have people on staff that must be trolling the social media of employees and when they find a conservative, or someone they believe to be, they attack,” Steele said.
Steele said female employees appear to be particular targets of the airlines, as they “appear to be isolated and intimidated for hours on end.”
Flint connected incidents such as those described above to political interests, telling The Defender the FAA approved COVID-19 vaccines for pilots just two days after the U.S. Food and Drug Administration (FDA) issued its first Emergency Use Authorization (EUA) for such vaccines, on Dec. 10, 2020.
“I thought to myself, how could the FAA analyze the data and determine it was safe for pilots in just two days, when it took the FDA months to go over the trial data?” Flint said.
Flint said that was an especially jarring development, in light of the increased risk that pilots and cabin crew face:
“I was also extremely curious to know how the FAA is so certain that this vaccine will be safe for pilots when it’s obvious that Pfizer did not do a trial solely on pilots to find out if it would cause some of the serious health problems that immediately started to show up once the mass vaccination campaign [began].”
In the process, Flint stated, the FAA violated its own regulations.
Under the Guide for Aviation Medical Examiners: Pharmaceuticals (Therapeutic Medications) Do Not Issue – Do Not Fly, the FAA has a long-standing rule that states:
“FAA requires at least one year of post-marketing experience with a new drug before consideration for aeromedical certification purposes. This observation allows time for uncommon, but aeromedically significant, adverse reactions to manifest themselves.”
Flint said it “became painfully obvious” the FAA issued this guidance based not on science or safety, but political reasons.
“Why did the FAA abandon its own rules by encouraging pilots to take a brand-new experimental drug?” Flint asked. “This action by the FAA was totally unprecedented and extremely dangerous.”
Providing an example of such danger, Flint said, “it is now widely reported that mRNA COVID-19 vaccines can cause blood clots,” adding that several peer-reviewed studies going back more than a decade “show pilots are approximately 60% more likely to experience blood clots due to the ‘nature of the job.’”
Supporting this assertion, on May 5, the FDA announced that it would restrict who could receive doses of the Johnson & Johnson COVID-19 vaccine, due to the risk of blood clots.
/snip RTWT at
Exclusive: Pilots Injured by COVID Vaccines Speak Out: ‘I Will Probably Never Fly Again’


































 Omicron sub-lineages BA.4 and BA.5
Omicron sub-lineages BA.4 and BA.5 Omicron sub-lineage BA.2.12.1
Omicron sub-lineage BA.2.12.1 The importance to maintain, and even enhance, surveillance and sequencing to track
The importance to maintain, and even enhance, surveillance and sequencing to track 





 Sheldon Yakiwchuk @YakkStack
Sheldon Yakiwchuk @YakkStack