Australian Medical Association vice-president Chris Moy has warned Aussies are like 'frogs being boiled slowly' as Covid death rates surge and hospitals struggle to cope with the third wave.

www.dailymail.co.uk
(fair use applies)
Top doctor says clueless Aussies are like 'frogs being boiled' in accepting Covid death amid fresh surge - as the ABC ramps up its campaign to bring back the most loathed lockdown rules
- Doctor says Aussies like 'frogs being boiled slowly' in latest wave of Covid
- Dr Chris Moy said health authorities were concerned about new sub-variants
- Dr Moy hit out at health minister Mark Butler for not reimposing mask mandates
- Mr Butler is repeatedly grilled by ABC journalists for failing to bring them back
- Australia's Covid death toll has surpassed 10,000 with over 4,000 hospitalised
By
Olivia Day For Daily Mail Australia
Published: 21:19 EDT, 10 July 2022 | Updated: 22:55 EDT, 10 July 2022
The Australian Medical Association has issued a dramatic
Covid-19 warning, telling the ABC that Aussies are like 'frogs being boiled slowly' into accepting current death numbers - as the ABC pushes strongly for the return of lockdown restrictions.
AMA vice-president Chris Moy told the ABC's News Breakfast on Monday that health authorities are more worried about Covid now than they have been for many months.
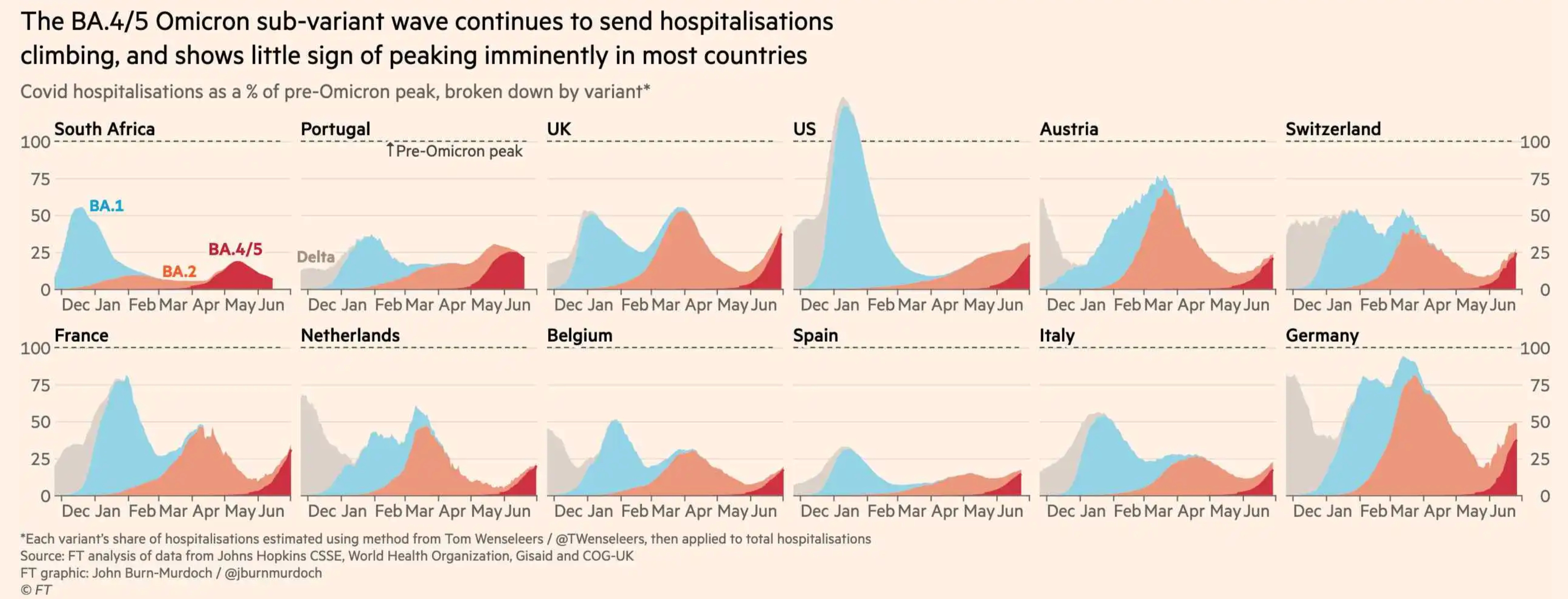
Doctors are worried about the rapid spread of the
BA.4 and BA.5 Omicron sub-variants, because they are 'more infectious, cause more reinfections and severe disease' and travel down the lungs.
The doctor blamed the federal election for giving the country a 'false sense of security' as politicians ended mask mandates and Covid restrictions to signal victory over the virus.
'Unfortunately to some degree, we've been like frogs boiled slowly and we're accepting this death rate which is continued on,' Dr Moy said.
He said there has been more than 10,200 deaths of people with Covid in their system over the past two and half years since the virus emerged.
Australia's most recent annual death toll from all causes is 160,000.
The top doctor's warning comes as the ABC appears to be spearheading a campaign for the return of hated Covid rules.
A succession of high-profile hosts have repeatedly questioned why masks are not being mandated across the country.
During his apperaance, Dr Moy urged Aussies to wear masks indoors and in high-risk scenarios for the next few months.
'Masks are very high impact in terms of benefit with low inconvenience compared to things like isolation, which we can encourage at the moment,' he said.
The doctor urged Australians worried about transmission during the third wave to get any vaccines or antiviral treatments they are eligible for.
Pensioners over 70 who test positive to the virus will be able to access antivirals on the Pharmaceutical Benefits Scheme from Monday. Two antivirals are on the PBS - Lagevrio and Paxlovi - with the announcement on Sunday expanding access and lowering cost for millions of Australians.
The pills normally cost more than $1,000, but will be available for $6.80 for concession card holders and around $40 for everyone else.
Dr Moy advised those experiencing symptoms like a runny nose, sore throat or cough to get a PCR test immediately and not rely on a RAT, where detection rates of the virus were only 60 per cent.
'Really consider wearing a mask in high-risk situations,' the doctor urged.
'Because what we need to do over the next 5-10 weeks, it's going to be a really high-risk period for us and we just don't want to overload the hospitals.'
Dr Moy called on Federal Health Minister Mark Butler to see 'what it's really like' for GP's on the frontline and claimed he was 'acting more like an economist'.
'We have been down this line before with the economists running this thing, and particularly New South Wales, and that didn't go very well in two outbreaks,' he said.
ABC hosts have repeatedly grilled the health minister over why he and his state counterparts aren't reintroducing mask mandates, given the rapid spread of Covid and winter viruses.
ABC News Breakfast presenter Michael Rowland on Friday accused Mr Butler of 'accepting' deaths by not re-introducing compulsory face-coverings.
Mr Butler said the advice from the chief health officers is that Australia has 'moved beyond the era of very broad mask mandates and lockdowns', and that you can 'make your own choice' about wearing a mask indoors.
But Mr Rowland refused to accept that answer, claiming that studies showed mask mandates offered close to a 100 per cent success rate - despite case numbers climbing even when previous mandates were enforced during the Delta and Omicron outbreaks.
We do know there are studies reflecting this, that compulsory mask mandates have close to 100% success rate,' Mr Rowland said.
'(That's) as opposed to what you're saying, just asking people to wear them. You're not worried about people not making the right decision here?'
Mr Butler fired back saying Australians, who have unrestricted access to vaccines to protect against serious illness, can 'take control of their own circumstances' in the third year of the pandemic.
Mr Rowland then pointed to the over 10,000 people who have died with the virus.
'By not taking steps to minimise transmissions ... aren't we, Mark Butler, as a society, implicitly accepting that death toll?' he said. 'And are you comfortable with that?'
Mr Butler attempted to answer the question, noting the lives 'tragically' lost before he was cut off by the television host.
'As a society, do we just sit back and accept that?' Rowland interrupted.
'No, we don't sit back and accept it,' the health minister hit back.
The health minister was similarly grilled by journalist David Speers during the ABC's Insiders program on Sunday.
Speers asked: 'You say we've moved to a new phase of the pandemic but you just told us we're in a new wave that's very serious, you're worried about this. Are we really in a new phase of the pandemic where we don't need to consider some of these old measures, like mask mandates, in particular?
'Why don't we look at that for the next six weeks?'
Mr Butler said he had received no advice to mandate masks and said face-coverings were better in 'targeted' areas like hospitals, airports and aged-care settings.
'And if you're in a crowding indoor space with no ability to socially distance you should give strong consideration to wearing a mask,' he added.
Speers said a recommendation that people wear a mask was 'ineffectual' with the proof seen in shopping centres or stadiums where few were worn.
'Wasn't one of the lessons of this pandemic, mask mandates for a fixed period, work?' he asked the health minister.
'But we're deep into the third year. They did work very well for the first couple of years,' Mr Butler replied to which the host hit back: 'We're in a third wave'.
Mr Butler said the government was getting advice that such mandates are best done in a targeted way and focusing on protecting vulnerable members of the population.
Meanwhile, Aussies over 30 have been urged to consider rolling up their sleeve for a fourth vaccine dose.
More than 37,000 new infections and 77 deaths were reported across the country on Saturday with Omicron variants BA.4 and BA.5 now the dominant strains of the virus.
Almost 42,000 cases were also announced nationally on Friday, the third 40,000-plus day in a row while the number of patients hospitalised with the virus tops 4,000, up by more than 1,000 in the past fortnight.


 www.bbc.com
www.bbc.com